

Apart from the more obvious gender differences like pregnancy and some aging-related conditions (e.g., osteoporosis, menopausal changes), how much thought is generally given to the anatomical and physiological differences between men and women when designing programs for female clients? A fair assumption might be very little considering the lack of available information, and the lack of attention paid to these differences.
Although anatomical differences at the knee have been long understood, programming that promotes good knee integrity is still inadequately emphasized in many female training programs. Recently, additional physiological differences between genders have been identified, yet continue to be neglected in programming (1-4). Although few anatomical and physiological differences exist between pre-pubescent males and females, following puberty, these differences become evident and merit consideration in design and training.
Enroll in the Women's Fitness program to learn even more about this topic!
Structural Differences:
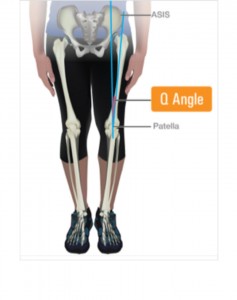
Perhaps the most cited gender difference relates to the fact that females normally have a wider pelvis (for childbearing purposes), which when coupled with shorter limb-lengths increases what is termed the Q-angle at the knee (Figure 1-1). The Q-angle is the measurement of the angle formed between the long axis of the femur bone (representing the quadriceps pull) and the long axis of the tibia (representing the patella tendon pull).
On average this angle deviation is approximately 17 – 18° in women, in comparison to 12 – 13° in men, but may be greater in women with wider hips and shorter limbs. The very nature of this deviation creates a potential weak link during basic (e.g., walking) and advanced movements (e.g., jump-landing).
Figure 1-1: Q-Angle at the Knee.
With females having smaller bones, ligaments, and muscles, which implies less surface area for attachment and support (integrity); and a more-narrow groove between the femoral epicondyles (bony structures at the lower end of the femurs) through which two major knee ligaments pass (anterior cruciate ligament - ACL and posterior cruciate ligament – PCL), this creates additional injury risks as these ligaments undergo more shearing during movement, especially during rotational-type movement between the femur and tibia.
Consider as well, gender-specific hormones (e.g., relaxin) and concentration levels which create greater joint laxity; and the slight gender difference in bone shape at the knee (upper part of tibia - tibial plateau is shorter and more rounded), and what you have is a greater potential for knee injuries in females, especially within the ACL (5). In fact, college-aged females suffer 2 – 6x the number of knee injuries playing the same sports as men, and approximately 70% of these ACL injuries occur in non-contact activities like jumping, jump-landing, stopping, and directional changes (6).
See also: Knee Strength for Females
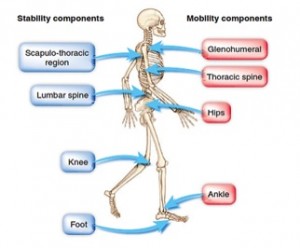
Within the upper extremity, men have broader shoulders to support more muscle mass, which in turn provides advantages to the muscles acting at the shoulders. This difference helps explain why woman only exhibit 52% of the strength of a man in the upper extremity versus 66% of the strength of a man in the lower extremity (7). So, how do these knee and shoulder disparities impact training? Given the popularity of higher-intensity, whole-body exercise-type programs (e.g., jumping exercises, squat-presses, cleans, etc.), it certainly justifies the need to first examine, then establish or improve knee and shoulder stability, before progressing to strengthen both regions, regardless of goals or training experience. Herein lies the value of a fitness professional well versed in assessing levels of stability and mobility within the lower extremity (ankle, knee and hip) and upper extremity (lumber/thoracic spine, scapula-thoracic region and glenohumeral joint) and throughout the entire kinetic chain. Keep in mind however, that these assessments also hold great value in men. Figure 1-2 provides a simplified overview of the stability-mobility relationship throughout the kinetic chain that the body follows during basic movement patterns (e.g., walking, bend-and-lift, push, pull, and rotation) (8). This illustration provides a template for professionals to follow when aiming to re-establish stability and mobility throughout the entire kinetic chain. Once assessed, any designed programs, whether corrective or active/functional in nature, should emphasize:
- Improvements to knee stability (strengthening the stability-mobility relationship between ankle-knee-hip); teaching proper squat and lunge mechanics (using body weight initially) and instructing jump-landing mechanics first if any power-type training is to be included.
- Improvements to shoulder stability before strengthening, following the individual stages of the NASM OPT ™ model. Sequentially, stability within the lumber spine (core stabilization) should precede mobility within thoracic spine region, which then helps promotes greater stability within the scapulo-thoracic region (i.e., controlling movement and position of shoulder blades against the ribcage), which provides a solid platform for effective glenohumeral push-pull movements.
Considering how many females now incorporate compound lifts and more ballistic-type movements (e.g., jumping) into their exercise routines, addressing these foundational needs in program design is certainly merited.
Figure 1-2: The stability-mobility relationship throughout the kinetic chain.
Bioenergetic Differences:
Traditional practices have always assumed that exercise intensity, duration, and conditioning level influence fuel utilization (i.e., fats or carbohydrates), but recent research has illustrated the significant role that gender plays within the energy pathways (1, 4). As women possess lower quantities of type II fibers than men (fibers responsible for anaerobic energy production) and because type I fibers store two to three times more fat than type II fibers, females are better suited at utilizing fats during exercise (11). The ovarian hormones (estradiol in particular – most biologically active form of estrogen) play a significant role upon fuel utilization during exercise (1, 4):
- Females utilize less glucose when compared to men during endurance-type (sub-maximal) exercise – perhaps a glycogen-sparing effect.
- Females have lower glycogen (carbohydrate) stores than men; estrogen also reduces carbohydrate-loading capacity – may impact training outcomes for endurance or ultra-endurance events.
- Females possess smaller fat droplets and more of them in muscle tissue in comparison to men – this facilitates greater fat access and transport into the mitochondria (sites where fats are burned for energy).
- Estrogen suppresses gluconeogenesis, which is the manufacture of glucose from non-carbohydrate stores like lactate and amino acids. This pathway becomes significant during sustained exercise or during glycogen-depleted states.
Likewise with anaerobic exercise, these same ovarian hormones negatively impact the energy pathways, which is significant given the popularity of HIIT-type workouts that rely predominantly upon these systems (1, 4, 9-10):
- Type II muscle fibers have greater quantities of creatine-phosphate (fuel substrate) and creatine kinase (key enzyme of the phosphagen system) – women have lower quantities of type II fibers.
- Key enzymes involved in glycolysis that metabolize glucose anaerobically (e.g., phosphorylase, PFK) are more active in men than women, implying slower rates of glycolysis and anaerobic energy production in women.
- Lower concentrations of the lactate dehydrogenase (enzyme responsible for pyruvate-lactate conversion) means less capacity to make lactate, and clear it and hydrogen ions into the blood from the working muscle. What this means is a lower lactate-generating capacity and lower tolerance for high-intensity anaerobic work.
- Smaller blood volumes also means reduced concentrations of lactate buffer in the blood – needed to tolerate lactate spillover from the exercising muscles.
Collectively, these factors diminish the overall efficacy and efficiency of the anaerobic pathways in women. So what does this all mean? Although no clear guidelines exist, the overall takeaways with respect to exercise is that females are:
- Better suited to lower-to-moderate, longer-duration, submaximal exercise.
- Better suited to continuous, steady-state exercise.
- Capable of performing intense anaerobic intervals, but the duration of the work bout should be shorter (up to approximately two minutes of true high-intensity as opposed to high-effort which is very different). Because females don’t produce as much lactate as men (which takes time to regenerate back to a usable fuel), the recovery intervals can be shorter than those with men (e.g., 1-to-2 work-to-recovery ratio versus a 1-to-3 work-to-recovery ratio for men).
An additional insight on gender differences pertains to arousal, which can impact exercise performance. Researchers examining sympathetic nervous responses (system responsible for our ‘fight-or-flight’ response) have observed lower activation of this response to stress and coined the phrase ‘tend-and-befriend’ instead (2, 12). Oxytocin is a hormone released from the pituitary gland that functions to initiate the letdown reflex during lactation and stimulates uterine contractions during childbirth, but also plays a significant role in social or affiliative (bonding) behaviors. Because of this hormone, females appear to demonstrate a diminished ‘fight-or-flight’ response when stressed. This response may decrease physical aggression and potential to engage as aggressively in physical activity as men.
Resistance Exercise Participation
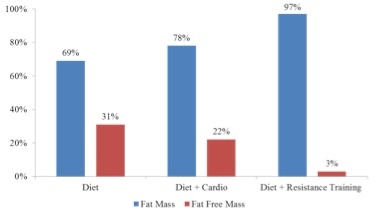
Table 1-1 provides the top reasons cited for participation in exercise by women of different age classifications (13). Whether reasons are to look better, lose weight, stay healthy or preserve functional strength, participation in resistance training is critical to the success of each. Effective strategies for weight loss should include resistance training as it minimizes potential losses of lean body mass as illustrated in Figure 1-3 (14).
Table 1-1: Reasons females participate in exercise.
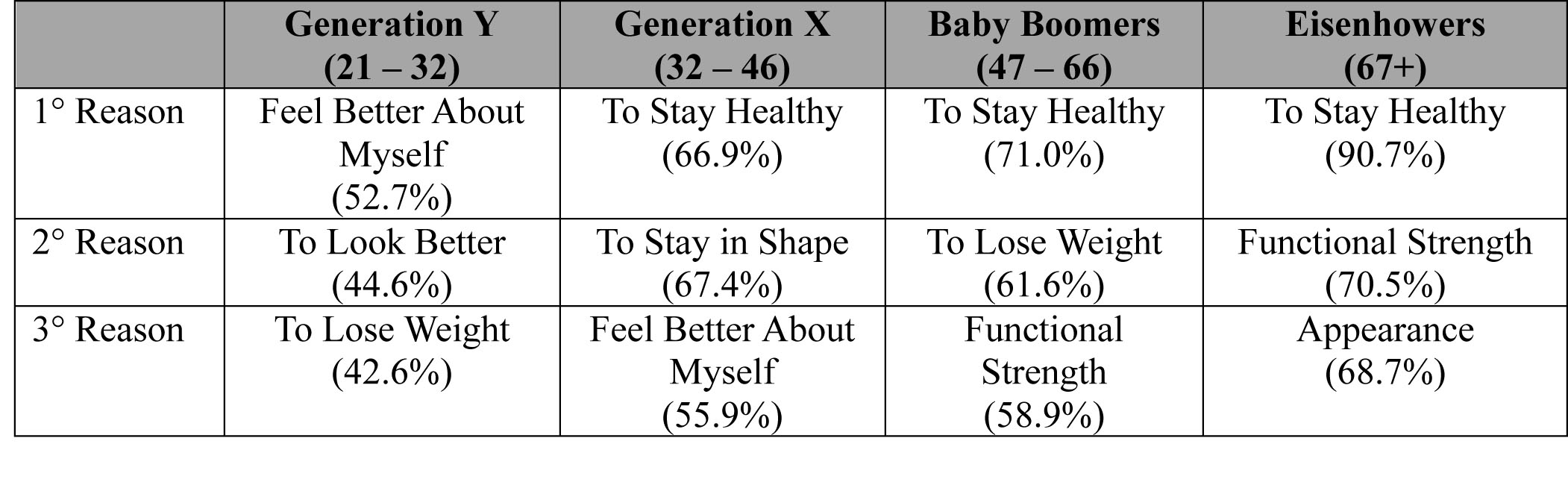
Figure 1-3: Compartmental losses in weight loss programs.
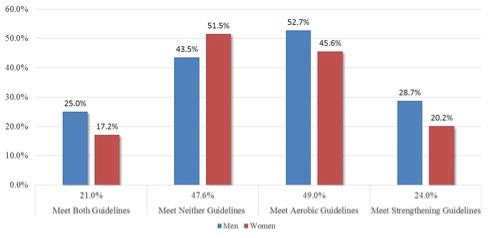
 As part of the 2008 Physical Activity Guidelines for Americans issued by the U.S. Department of Health and Human Services (HHS), adults should participate in moderate or high-intensity muscle-strengthening activities on two or more days a week (15). Unfortunately, participation by females in resistance-type activity appears to fall very short of that guideline as illustrated in Figure 1-4 (16). Social physique anxiety (i.e., fear of bulking up) is a common reason cited by women for not participating weight training, but so too are lack of knowledge and understanding on programming and technique. Social physique anxiety tends to be higher in women who exercised in a mixed-sex facility and results in shortened workouts. In this case, consider training these female clients in more secluded areas or during low-traffic times. Emphasize the development of skill and competence (self-efficacy) initially using selectorized machines which are generally a good fit.
As part of the 2008 Physical Activity Guidelines for Americans issued by the U.S. Department of Health and Human Services (HHS), adults should participate in moderate or high-intensity muscle-strengthening activities on two or more days a week (15). Unfortunately, participation by females in resistance-type activity appears to fall very short of that guideline as illustrated in Figure 1-4 (16). Social physique anxiety (i.e., fear of bulking up) is a common reason cited by women for not participating weight training, but so too are lack of knowledge and understanding on programming and technique. Social physique anxiety tends to be higher in women who exercised in a mixed-sex facility and results in shortened workouts. In this case, consider training these female clients in more secluded areas or during low-traffic times. Emphasize the development of skill and competence (self-efficacy) initially using selectorized machines which are generally a good fit.
Figure 1-4: Current participation rates in 2008 Physical Activity Guidelines for Americans.
 Although most fitness professionals are competent in discussing the multiple benefits of resistance training to women, the real challenge lies with asking the right questions, and then listening to, and understanding the apprehensions and barriers or pre-existing attitudes or belief systems that may hinder voluntary participation. Women who generally exercise for weight loss, toning and aesthetics often demonstrate lower levels of self-esteem and body satisfaction in comparison to women who exercise to improve mood, health and enjoyment. Consider exploring deeper reasons connected to health and moods rather than simply aesthetics and weight loss.
Although most fitness professionals are competent in discussing the multiple benefits of resistance training to women, the real challenge lies with asking the right questions, and then listening to, and understanding the apprehensions and barriers or pre-existing attitudes or belief systems that may hinder voluntary participation. Women who generally exercise for weight loss, toning and aesthetics often demonstrate lower levels of self-esteem and body satisfaction in comparison to women who exercise to improve mood, health and enjoyment. Consider exploring deeper reasons connected to health and moods rather than simply aesthetics and weight loss.
Finally, for those female clients comfortable with resistance-training, but focused upon toning and shaping rather than building muscle mass (difficult to do considering how females have only 5 – 10% of the testosterone of their male counterparts), programs should follow some simple guidelines (17):
- Target higher caloric burn rates through greater work rates (volume), but always incorporate appropriate, but minimal recovery intervals that don’t compromise technique or planned intensity.
- Superset (e.g., NASM OPT™ Phase 2 – Strength Endurance) or vertical loading (circuit) formats.
- Target more multi-joint, compound-type exercises as opposed to muscle isolation.
- Target larger type II fibers that demonstrate greater potential for growth – any addition of muscle mass increases resting metabolic rates which promote faster weight loss or weight maintenance. Type II fibers are optimally targeted with load (requires longer recovery intervals which diminishes caloric burn rate) or with power (explosive movements):
- Implement slower, controlled eccentric movements to trigger some muscle damage.
- Implement more explosive concentric movements to recruit the larger type II fibers.
- Utilize appropriate loads that ensure sustained work rates without compromise to proper form.
- Phase 5 of the NASM OPT™ model, 30 – 45% of 1RM or 10% of body weight are recommended.
The information contained within this article provides only some of the essential differences that exist between the genders. These ideas and others should always be carefully considered when programming for female clients to optimize the overall training experience and the opportunity to attain any desired outcomes.
References:
- Tarnopolosky, M.A. (2008). Sex differences in exercise metabolism and the role of 17-beta estradiol. Medicine and Science in Sports and Exercise, 40(4), 648-654.
- Sapolsky RM, (2004). Why Zebras don’t get ulcers. New York, NY: Henry Holt and Company, LLC.
- Moghadasi, M. and Siavashpour, S. (2013). The effect of 12 weeks of resistance training on hormones of bone formation in young sedentary women. European Journal of Applied Physiology, 113, 25-32.
- Oosthuyse, T. and Bosch, A.N. (2010). The effect of menstrual cycle on exercise metabolism. Sports Medicine, 40(3), 207-227.
- Wahl CL, (2012). An Association of Lateral Knee Sagittal Anatomic Factors with Non-Contact ACL Injury: Sex or Geometry? The Journal of Bone and Joint Surgery (American), 94(3):217-226.
- Arendt E, and Dick R (1995). Knee injury patterns among men and women in collegiate basketball and soccer. American Journal of Sports Medicine, 23(6):694-701.
- Miller AE, MacDougall JD, Tarnopolsky MA, and Sale DG, (1993). Gender differences in strength and muscle fiber characteristics. European Journal of Applied Physiology and Occupational Physiology, 66(3):254-262.
- Bryant CX, and Green DJ (eds.) (2010). ACE Personal Trainer Manual (4th edition). San Diego, CA, American Council on Exercise.
- Kenney WL, Wilmore JH, and Costill DL, (2012). Physiology of Sport and Exercise (5th edition). Champaign, IL: Human Kinetics.
- McArdle WD, Katch FI, and Katch VL, (2015). Exercise Physiology; Nutrition, Energy and Human Performance. Baltimore, MD: Wolter Kluwer Health – Lippincott, Williams & Wilkins.
- Shaw CS, Clark J, and Wagenmakers AJM, (2010). The effect of exercise and nutrition on intramuscular fat metabolism and insulin sensitivity. Annual Review for Nutrition. 30:13-34.
- Taylor SE, Klein LC, Lewis BP, Gruenewald TL, Gurung RAR, and Updegraff JA, (2000). Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychological Review, 107(3): 411-429.
- Leisure Trends Group, (2012). The IHRSA Trend Reports, May/August 2012, Boulder, CO.
- Stiegler P, and Cunliffe A, (2006). The Role of diet and exercise for the maintenance of fat-free mass and resting metabolic rate during weight loss. Sports Medicine, 36(3): 239-263.
- Office of Disease Prevention and Health Promotion / U.S. Department of Health and Human Services, (2008). 2008 Physical Activity Guidelines for Americans. http://www.health.gov/paguidelines/guidelines/summary.aspx. Retrieved 01/10/15.
- Centers for Disease Control and Prevention (2011). Adult Participation in Aerobic and Muscle-Strengthening Physical Activities — United States, 2011. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6217a2.htm Retrieved 01/10/15.
- Clark MA, Sutton BG, and Lucett SC, (Editors) (2014). NASM Essentials of Personal Fitness Training (4th edition revised). Burlington, MA, Jones & Bartlett Publishing.














