

Are your swimming clients at risk for Swimmer’s Shoulder? The repetitive overhead movements, combined with faulty stroke mechanics and postural distortion patterns can place the shoulder joint in a risky position. Put the NASM Corrective Exercise Continuum to work for you and your clients to keep them in the swim all year long!
The shoulder complex is one of the most complex joints of the human body. It consists of articulations between the sternum, clavicle, humerus, scapula, and rib cage. The inclusion of overhead activities into one’s fitness activities such as throwing or swimming can put undue stress on these structures that may potentially lead to various overuse injuries.
With over 50 million Americans enjoying swimming recreationally, and the growing popularity shown through rising annual memberships for swimming and triathlon programs, these overuse injuries may experience a similar increase in prevalence (1,2,3). The current range of shoulder pain reported by swimmers is 40-91% (4).
One example of such an overuse injury is Swimmer’s Shoulder. Swimming as a movement requires repeated glenohumeral circumduction and competitive swimmers typically exceed 4,000 strokes per shoulder in a single workout! This figure alone lays basis for swimmers being vulnerable to, and a common source of shoulder injury and discomfort (5,6).
What is swimmer's Shoulder?
In broad terms, Swimmer’s Shoulder can best be described as impingement caused by excessive glenohumeral movement through the glenoid fossa. The excess movement is caused by laxity in the shoulder capsule leading to anterior instability, and in turn, the repeated, non-optimal circumduction causes compression in the subacromial space.
Also read: Enhancing Scapular Stabilization.
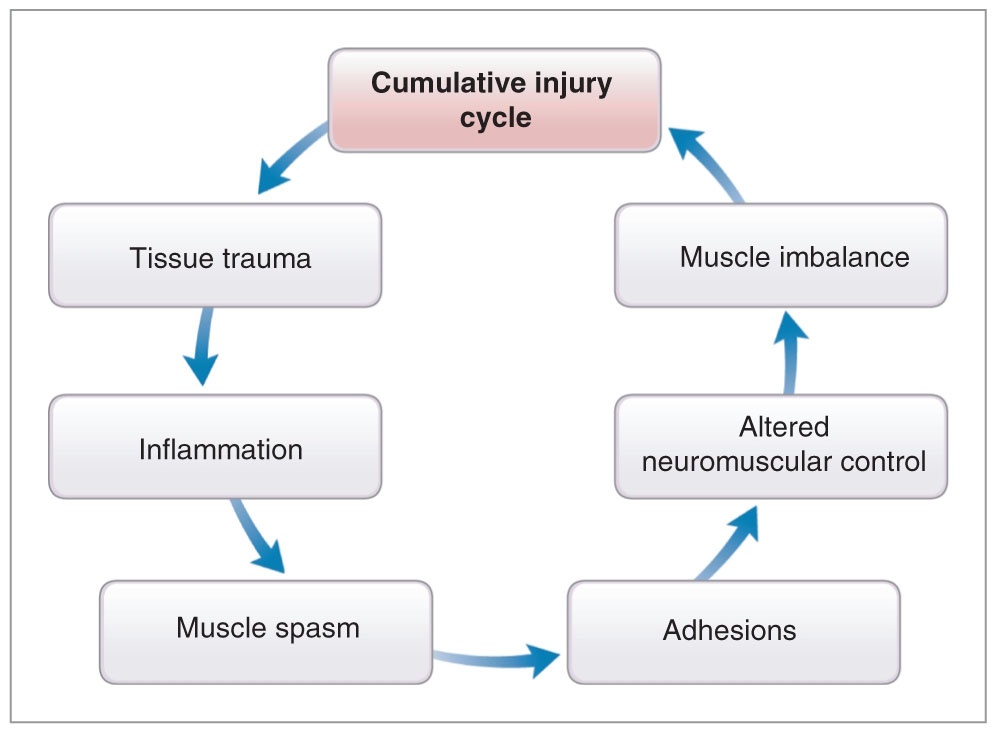
Postural distortion patterns such as upper crossed syndrome and faulty swim technique can further predispose someone to this injury (5,6,7). In addition, fatigue and the resulting swim-stroke adjustment to remain pain free further push this injury into a cycle of dysfunction (5).
To prevent overuse injury from swimming, one of the most prudent things to do is take a pro-active approach to prevention by using the principles of corrective exercise. Through a subjective and visual assessment, one can quickly screen those who may be predisposed to Swimmer’s Shoulder (7).
Is the client an office worker? Is the client an overhead athlete? Does the client present with forward head and/or rounded shoulder posture? Further utilizing a thorough assessment to evaluate passive and active range of motion allows professionals to address and correct existing, or pro-actively prevent muscle imbalances that may create a disposition towards Swimmer’s Shoulder.
An example of training for shoulder impingement
As an example, let’s consider a client who works 40-50 hours per week in an office setting and is also a recreational triathlete. It is immediately evident he presents with forward head posture and slightly rounded shoulders. Further assessments consist of goniometric (range of motion, see chart) and transitional movements. Specifically, shoulder flexion and glenohumeral internal/external rotation, the overhead squat, wall horizontal abduction, rotation, and shoulder flexion tests.
The most prudent of practitioners should take the assessment a step further with manual muscle testing of the rotator cuff muscles, rhomboids, lower trapezius, and serratus anterior. Manual muscle testing serves as confirmation for the findings of the range of motion and transitional movement assessments. With the compensations seen, the practitioner can begin forming a framework for the corrective exercises the client requires (Table 1).
Table 1
| Static Posture | Upper Crossed Syndrome (rounded shoulders, forward head posture) |
| Goniometric Assessment | Decreased shoulder flexionDecreased glenohumeral internal and/or external rotation |
| Overhead Squat | Arms fall forward |
| Horizontal Abduction Wall Test | Elbows flexShoulders elevate |
| Rotation Wall Test | Shoulders elevate |
| Shoulder Flexion Wall Test | Shoulders elevate |
| Pushing, Pulling, or Pressing Assessments | Shoulders elevateForward head |
| Manual Muscle Testing | Middle and lower trapezius, rhomboids, and rotator cuff muscles tested weak |
A corrective exercise program based on NASM methodology should involve exercises to inhibit and lengthen the overactive musculature, activate the inhibited musculature, and finally integrate by enhancing functional capacity through multiplanar neuromuscular control (7). 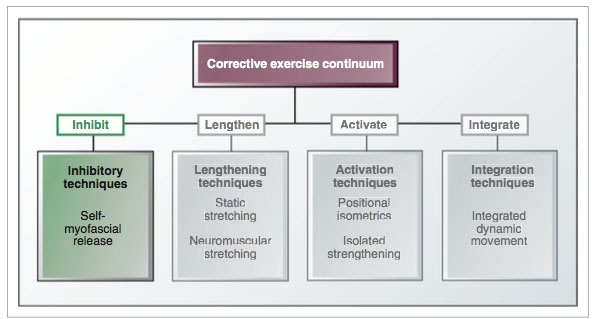
Table 2 provides a sample workout using the NASM Corrective Exercise Continuum based on the findings of the sample assessment provided earlier.
Table 2
| INHIBIT | Sets | Time | Notes |
| Self-myofascial Release | |||
| Upper Trapezius | 2 | 30s | Use Theracane, tennis ball, etc. |
| Pectoralis Major | 2 | 30s | Use Theracane, tennis ball, etc. |
| Latissimus Dorsi | 2 | 30s | Foam Roller |
| Thoracic Spine | 2 | 30s | Foam Roller |
| LENGTHEN | Sets | Time | Notes |
| Upper Trapezius | 2 | 30s | Static Stretching |
| Pectoralis Major | 2 | 30s | Static Stretching |
| Latissimus Dorsi | 2 | 30s | Static Stretching |
| ACTIVATE | Sets | Reps | Tempo | Notes |
| Ball Combo II with Dumbbells (middle/lower trapezius, rhomboid, rotator cuff) | 1 | 10-15 | 2s isometric hold4s eccentric | Isolated Strengthening |
| INTEGRATE | Sets | Reps | Tempo | Notes |
| Squat to Row | 1 | 10-15 | Controlled | |
| Single-leg Romanian Deadlift with PNF Pattern | 1 | 10-15 | Controlled |
A comprehensive corrective exercise program based on NASM’s scientifically-based methodologies puts fitness professionals ahead of the curve when working with clients that exhibit movement compensations and dysfunction. Further, utilizing corrective exercise as a preventative tool may also have positive results in reducing the risk for these injuries (7).
For an additional resource on protecting your clients' shoulders, watch this video!
REFERENCES:
- Participation in Selected Sports Activities: 2009. U.S. Census Bureau.
- Membership demographics for the 2014 membership year. USA Swimming. http://www.usaswimming.org Accessed July 10, 2015
- Membership demographics for the 2013 membership year. USA Triathlon. http://www.usatriathlon.org/about-multisport/demographics.aspx Accessed July 10, 2015
- Tate A, Turner GN, Knab SE, Jorgensen C, Strittmatter A, Michener LA. Risk Factors Associated With Shoulder Pain and Disability Across the Lifespan of Competitive Swimmers. J Athl Train. 2012 Mar-Apr; 47(2): 149–158.
- Tovin BJ. Prevention and Treatment of Swimmer's Shoulder. N Am J Sports Phys Ther. 2006 Nov; 1(4): 166–175.
- Heinlein SA, Cosgarea AJ. Biomechanical Considerations in the Competitive Swimmer’s Shoulder. Sports Health. 2010 Nov; 2(6): 519–525.
- Clark MA, Lucett SC. NASM Essentials of Corrective Exercise. 1st ed. Philadelphia, PA. Lippincott Williams & Wilkins; 2011.














