


Within the first part of this three-part series, the benefits of using joint range of motion (ROM) testing to confirm the findings of both the static and dynamic postural assessments, as well as mobility assessments, were discussed.
To reiterate, the fitness professional may be able to determine possible muscular imbalances (i.e., overactive/shortened and underactive/lengthened muscles) by performing both static and dynamic postural assessments.
However, the fitness professional can only indeed confirm if muscles are in an overactive/shortened state through performing specific mobility assessments, like those provided in the updated Corrective Exercise Specialization (CES) certification course, as well as Chapter 10 of the certification textbook resource Essentials of Corrective Exercise Training (2nd ed.).
Unfortunately, the mobility assessments included in the CES certification course and textbook provide only benchmarks through visually assessing ROM (e.g., the knee extending to nearly or entirely straight without compensation during the active knee extension test) (National Academy of Sports Medicine, 2022), as opposed to objectively measuring ROM (e.g., 15 degrees of knee flexion) using a measurement device such as a goniometer or inclinometer.
By objectively measuring ROM, the fitness professional can ensure that muscular imbalances and limited ROM exist and witness objective improvements in ROM over time by designing and implementing a proper individualized corrective exercise program and periodically reassessing the client. Clients enjoy seeing objective improvements and progression in their fitness level when working with a fitness professional.
Therefore, showing actual numerical improvements in ROM can assure clients that corrective exercise training programs have provided tangible benefits that can transfer into the decreased risk of both acute and chronic overuse injuries and improvements in performance both on and off the field/court.
USING A SMARTPHONE APPLICATION TO MEASURE ROM VS. GONIOMETER OR INCLINOMETER
As previously mentioned in part one of this series, the proper use of both a goniometer and inclinometer to measure ROM requires many hours of learning and practical experience under a trained professional and is commonly part of the course curriculum in college degree programs such as kinesiology, exercise science, athletic training, and physical therapy.
However, the fitness professional is not required to be a licensed professional (e.g., athletic trainer or physical therapist) to measure active ROM and passive ROM using gravity, such as the modified Thomas test or prone passive hip internal rotation test. Please be aware that it may be outside of the fitness professional’s scope of practice to utilize manual manipulation to passively move the client’s joints through a passive ROM to obtain a measurement (e.g., the fitness professional actively moving the client’s knee into further extension during the active knee extension test). Legal regulations may vary from state to state.
Over the last decade or so, the use of smartphone applications (e.g., Clinometer + Bubble Level) is a valid and reliable tool for measuring ROM compared to using a goniometer and inclinometer (Keogh et al., 2019; Wellmon et al., 2016). In addition, the use of a smartphone application is efficient because most individuals carry smartphones with them, whereas not every individual owns or carries a goniometer or inclinometer.
Moreover, using a smartphone application to measure ROM may be viewed as a more straightforward method of measuring ROM than goniometry. This is because a goniometer is comprised of a) an axis (A) or fulcrum that must be accurately aligned with the imaginary joint line or axis of rotation for the joint being measured (e.g., the tibiofemoral or knee joint during the active knee extension test), b) stationary/stabilization arm (SA) that must be accurately aligned with the nonmoving limb or bony segment (e.g., the lateral midline of the femur), and c) a movement arm (MA) that must be accurately aligned with the moving limb and is the only moving component of the goniometer (National Academy of Sports Medicine, 2014)
(Figure 1). The smartphone itself serves as the MA, and therefore, the fitness professional does not need to be concerned with properly aligning the A or SA of the goniometer.
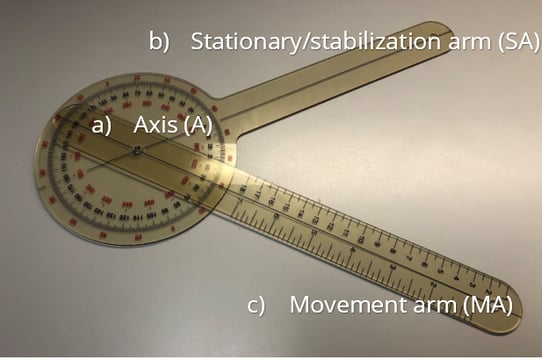
Figure 1. Goniometer with the a) axis (A), b) stationary/stabilization arm (SA), and c) movement arm (MA) labeled
MEASURING LOWER EXTREMITY RANGE OF MOTION USING A SMARTPHONE APPLICATION
Note: Please provide instructions and demonstrate each test before testing the client.
Ankle Dorsiflexion (Weight Bearing Lunge with Knee Flexed)
Instructions for measuring ROM: Have the client face a wall in a lunge position with shoes off, feet straight ahead, heels planted flat on the ground, and the client’s hands against the wall. You will measure the front ankle (i.e., the test leg) with the knee flexed for dorsiflexion ROM. Have the client start with their big toe approximately 2 inches from the wall and flex the front knee in an attempt to touch the wall with their front knee without any compensation at the foot (i.e., overpronation/flattening of the foot) and/or knee (i.e., knee valgus/inward or valgus/outward movement) (National Academy of Sports Medicine, 2022).
If the client cannot touch the wall with the front knee without the heel rising or shows compensations, have the client move the foot approximately one inch closer to the wall or until the heel does not rise and prepare for measurement. If the client can touch the wall with their front knee with no compensations, have the client progressively move the front foot backward until the knee can no longer touch the wall without the heel rising or any compensations. At the point where the heel is just about to rise with no compensations is the end range of dorsiflexion ROM.
Set the smartphone application to 0 degrees while in the horizontal position and place the smartphone horizontally just above the superior aspect of the calcaneus (Banwell et al.,2019) (Figure 2). Measure to the nearest degree or tenth of a degree and repeat on the opposite leg.

Figure 2. Ankle Dorsiflexion (Weight Bearing Lunge with Knee Flexed)
Normal ROM: No known normative values; asymptomatic individuals may show approximately 30 degrees of dorsiflexion (Banwell et al., 2019)
Overactive/shortened muscle/s if ROM is restricted: Plantar flexors (specifically the soleus)
Ankle Dorsiflexion (Weight Bearing Lunge with Knee Extended)
Instructions for measuring ROM: Have the client face a wall in a lunge position with shoes off, feet straight ahead, heels planted flat on the ground, and the client’s hands against the wall. You will measure the rear ankle (i.e., the test leg) with the knee in full extension for dorsiflexion ROM. Have the client start with their hind foot as far back as possible with the heel flat and no compensation at the foot (i.e., overpronation/flattening of the foot) or knee (i.e., knee valgus/inward movement). Have the client progressively move the rear foot backward until the heel rises or any compensations occur. At the point where the heel is just about to rise with no compensations is the end range of dorsiflexion ROM. Set the smartphone application to 0 degrees while in the horizontal position and place the smartphone horizontally just above the superior aspect of the calcaneus (Banwell et al., 2019) (Figure 3). Measure to the nearest degree or tenth of a degree and repeat on the opposite leg.

Figure 3. Ankle Dorsiflexion (Weight Bearing Lunge with Knee Extended)
Normal ROM: No known normative values; asymptomatic individuals may show approximately 30 degrees of dorsiflexion (Banwell et al., 2019)
Overactive/shortened muscle/s if ROM is restricted: Plantar flexors (specifically the gastrocnemius)
Active Knee Flexion (Duncan-Ely Test)
Instructions for measuring ROM: Have the client lay in a prone position on a table or the floor. Have the client actively flex or bend their right knee (i.e., the test leg) as much as possible, bringing their heel towards their buttocks without lifting their right hip off the table or floor. Set the smartphone application to 0 degrees while in the horizontal position and place the smartphone at the middle third of the anterior region of the tibia (Dos Santos et al. 2017) (Figure 4). Please note, an additional fee may be required for the updated version of the Clinometer + Bubble Level smartphone application that reads beyond 90 degrees (i.e., 90 to 360 degrees). Measure to the nearest degree or tenth of a degree and repeat on the opposite leg.

Figure 4. Active Knee Flexion (Duncan-Ely Test)
Normal ROM: 135-150 degrees of knee flexion (American Medical Association, 1988; Greene & Heckman, 1994)
Overactive/shortened muscle/s if ROM is restricted: Quadriceps complex
Active Knee Extension
Instructions for measuring ROM: Have the client lay in a supine position on a table or the floor. Ask the client to actively flex their right hip to 90 degrees of flexion and grab behind the right thigh just above the knee with both hands to stabilize the right hip at 90 degrees of flexion. Have the client then actively extend or straighten their right knee (i.e., the test leg) as far as possible keeping their ankle in a neutral position and without the right hip moving into extension or the left hip moving into flexion.
Set the smartphone application to 0 degrees while in the vertical position and place the smartphone at the middle third of the anterior region of the tibia (Dos Santos et al., 2017) (Figure 5). Measure to the nearest degree or tenth of a degree and repeat on the opposite leg.

Figure 5. Active Knee Extension
Normal ROM: 0-10 degrees of knee flexion (American Medical Association, 1988; Greene & Heckman, 1994)
Overactive/shortened muscle/s if ROM is restricted: Hamstring complex, gastrocnemius
MEASURING LUMBO-PELVIC-HIP COMPLEX RANGE OF MOTION USING A SMARTPHONE APPLICATION
Passive Hip Extension and Knee Flexion (Modified Thomas Test)
Instructions for measuring ROM: Have the client sit at the very end of a table and slowly lay back while grabbing both knees and pulling them into their chest. With consent to touch the client, please support the client’s back as they lay back into a supine position to prevent injury. Have the client then let go of their right leg (i.e., the test leg), allowing gravity to naturally pull their right hip into extension and right knee into flexion, while still holding their left knee near their chest in hip and knee flexion. The right hip and knee should be in a relaxed position during measurement.
To measure hip extension, set the smartphone application to 0 degrees while in the horizontal position and place the smartphone in the middle of the lateral aspect of the right thigh aligned with the femur. Have the earpiece at the top of the phone in line with the right hip joint and the phone button or middle of the bottom part of the phone in line with the middle of the knee joint (Clapis, Davis, & Davis, 2008) (Figure 6).

Figure 6. Passive Hip Extension (Modified Thomas Test)
Measure to the nearest degree or tenth of a degree. To measure knee flexion, keep the smartphone application set to 0 degrees while in the horizontal position and place the smartphone at the middle third of the anterior region of the tibia (Dos Santos et al. 2017) (Figure 7).

Figure 7. Passive Knee Flexion (Modified Thomas Test)
Measure to the nearest degree or tenth of a degree. Have the client bring the right leg back up to the start position next to their left leg and grab the right knee. Then have the client let go of their left leg, allowing gravity to naturally pull their left hip into extension and left knee into flexion, while still holding their right knee near their chest in hip and knee flexion. Repeat measurement of hip extension and knee flexion on the left side.
Normal ROM: 0-10 degrees of hip extension (Greene & Heckman, 1994)
Overactive/shortened muscle/s if ROM is restricted: Iliopsoas
Normal ROM: 90 degrees of knee flexion (National Academy of Sports Medicine, 2022)
Overactive/shortened muscle/s if ROM is restricted: Rectus femoris (and other muscles of quadriceps complex)
Prone Passive Hip Internal Rotation
Instructions for measuring ROM: Have the client lay in a prone position on a table or the floor. Have the client bring their legs together and flex or bend both knees to 90 degrees. Ask the client to then allow gravity to pull their feet apart to the sides simultaneously as far as possible causing both hips to move into internal rotation, while still maintaining 90 degrees of knee flexion at both knees and the front of the hips remaining on the table or floor.
Set the smartphone application to 0 degrees while in the vertical position and place the smartphone on the anterior region of the right tibia with the bottom of the phone just below the tibial tuberosity (i.e., the test leg) (Charleton et al., 2015). Have the earpiece at the top of the phone in line with the middle of the ankle joint and the phone button or middle of the bottom part of the phone in line with the middle of the knee joint (Figure 8). Measure to the nearest degree or tenth of a degree and repeat on the left leg.

Figure 8. Prone Passive Hip Internal Rotation
Normal ROM: 40-45 degrees of internal rotation (American Medical Association, 1988; Greene & Heckman, 1994)
Overactive/shortened muscle/s if ROM is restricted: Hip external rotators
Seated Active Hip Internal Rotation
Instructions for measuring ROM: Have the client sit at the end of a table in an upright posture, their hips in a neutral position, and their knees flexed at a 90-degree angle. Have the client actively internally rotate their right hip (i.e., the test leg) by moving their right foot up and away from the midline as far as possible, without hiking their hip, abducting their hip, laterally flexing, flexing, or extending at their spine (National Academy of Sports Medicine, 2022).
Set the smartphone application to 0 degrees while in the vertical position and place the smartphone on the anterior region of the right tibia with the top of the phone just below the tibial tuberosity (i.e., the test leg) (Charleton et al., 2015). Have the earpiece at the top of the phone in line with the middle of the knee joint and the phone button or middle of the bottom part of the phone in line with the middle of the ankle joint (Figure 9). Measure to the nearest degree or tenth of a degree and repeat on the left leg.

Figure 9. Seated Active Hip Internal Rotation
Normal ROM: 40-45 degrees of internal rotation (American Medical Association, 1988; Greene & Heckman, 1994)
Overactive/shortened muscle/s if ROM is restricted: Deep hip external rotators (Piriformis, gemellus superior, gemellus inferior, obturator externus, obturator internus, quadratus femoris), iliopsoas, gluteus maximus, gluteus medius – posterior fibers, and biceps femoris.
Seated Active Hip External Rotation
Instructions for measuring ROM: Have the client sit at the end of a table in an upright posture, their hips in a neutral position, and their knees flexed at a 90-degree angle. Have the client actively flex the left knee bringing the left foot under the table to allow for external rotation of the right hip. If there is no room under the table to allow for knee flexion, have the client actively extend the left knee to allow for external rotation of the right hip.
Have the client then actively externally rotate their right hip (i.e., the test leg) by bringing their right foot across the midline of the body as far as possible, without hiking their hip, abducting their hip, laterally flexing, flexing, or extending at their spine (National Academy of Sports Medicine, 2022). Set the smartphone application to 0 degrees while in the vertical position and place the smartphone on the anterior region of the right tibia with the top of the phone just below the tibial tuberosity (Charleton et al., 2015).
Have the earpiece at the top of the phone in line with the middle of the knee joint and the phone button or middle of the bottom part of the phone in line with the middle of the ankle joint (Figure 10). Measure to the nearest degree or tenth of a degree and repeat on the left leg.

Figure 10. Seated Active Hip External Rotation
Normal ROM: 45-50 degrees of external rotation (American Medical Association, 1988; Greene & Heckman, 1994)
Overactive/shortened muscle/s if ROM is restricted: Tensor fascia latae, gluteus minimus, gluteus medius – anterior fibers, semitendinosus, semimembranosus, and hip adductors
References:
- American Medical Association (1988). Guides to the evaluation of permanent impairment (3rd ed.). American Medical Association.
- Banwell, H. A., Uden, H., Marshall, N., Altmann, C., & Williams, C. M. (2019). The iPhone measure app level function as a measuring device for the weight bearing lunge test in adults: A reliability study. Journal of Foot and Ankle Research, 12(1), 1–7. https://doi.org/10.1186/s13047-019-0347-9
- Charlton, P. C., Mentiplay, B. F., Pua, Y.-H., & Clark, R. A. (2015). Reliability and concurrent validity of a Smartphone, bubble inclinometer and motion analysis system for measurement of hip joint range of motion. Journal of Science and Medicine in Sport, 18(3), 262. https://doi.org/10.1016/j.jsams.2014.04.008
- Clapis PA, Davis SM, & Davis RO. (2008). Reliability of inclinometer and goniometric measurements of hip extension flexibility using the modified Thomas test. Physiotherapy Theory & Practice, 24(2), 135–141. https://doi.org/10.1080/09593980701378256
- Dos Santos, R. A., Derhon, V., Brandalize, M., Brandalize, D., & Rossi, L. P. (2017). Evaluation of knee range of motion: Correlation between measurements using a universal goniometer and a smartphone goniometric application. Journal of Bodywork & Movement Therapies, 21(3), 699–703. https://doi.org/10.1016/j.jbmt.2016.11.008
- Greene, W. B., & Heckman, J. D. (1994). The clinical measurement of joint motion. American Academy of Orthopedic Surgeons.
- Keogh, J. W. L., Cox, A., Anderson, S., Liew, B., Olsen, A., Schram, B., & Furness, J. (2019). Reliability and validity of clinically accessible smartphone applications to measure joint range of motion: A systematic review. PloS One, 14(5), 1-24. https://doi.org/10.1371/journal.pone.0215806
- National Academy of Sports Medicine (2014). NASM essentials of corrective exercise training (1st ed. revised). Jones & Bartlett Learning.
- National Academy of Sports Medicine (2022). NASM essentials of corrective exercise training (2nd ed.). Jones & Bartlett Learning.
- Wellmon, R. H., Gulick, D. T., Paterson, M. L., & Gulick, C. N. (2016). Validity and Reliability of 2 Goniometric Mobile Apps: Device, Application, and Examiner Factors. Journal of Sport Rehabilitation, 25(4), 371–379. https://doi.org/10.1123/jsr.2015-0041
Student in Figures: Darcel Tinner (Health & Human Performance major)
Student Photographer: Dana Timpson (Exercise Science major)
ROM Tester in Figures: Dr. Ryan R. Fairall














