

Most clients, and exercise experts alike, use the term “tight” to indicate that a muscle or other form of contractile tissue is shorter than it should be. After being in the fitness industry for more than 15 years, I've heard the phrase “my piriformis is tight” at least 17 billion times (Granted, this could be an exageration, but the number is probably still close).
However, most clients are referring to a particular “feeling” as a muscle or tissue may feel tight, but this doesn’t always mean it is actually short.
The piriformis is one of those tricky muscles that doesn’t always correctly communicate its needs. This article will briefly explore the anatomy of the piriformis and present key movement characteristics that are much more telling and lead to better results than simple perceptions.
Within, we will explore corrective exercise principles that will help you make accurate assessments of the piriformis. A lot of the exercise prescription that we use can be strategically applied as a flexibility and stretching coach.
a definition of the piriformis
The piriformis is an external rotator of the hip that attaches proximally to the anterior surface of the sacrum and inserts onto the superior aspect of the greater trochanter. The near horizontal alignment of the muscle is what causes it to be a primary rotator. Also, the insertion at the top of the greater trochanter allows the muscle to serve as a secondary hip abductor.
As with most muscles, there is more than meets the eye when it comes to the function of the piriformis. Yes, it is an external rotator and hip abductor … in the anatomic position of 0⁰ of hip extension; 0⁰ of hip flexion; 0⁰ of adduction; 0⁰ of abduction; 0⁰ of internal rotation and 0⁰ of external rotation (Reynolds & Schrattenholzer, 2007).
However, neutral is very rare in the real world. As the hip moves, the function of the hip muscles change. When the hip is at about 45⁰ of flexion (Fig. 1), the line of pull of the piriformis now makes it act as a purely frontal plane muscle (abduction) with little to no transverse plane influence (Reynolds & Schrattenholzer, 2007).
 Fig. 1
Fig. 1
As the squat depth increases, the line of pull of the piriformis continues to change. Past 90⁰ the piriformis becomes an internal rotator of the hip (Neumann, 2010, Fig. 2).
 Fig. 2
Fig. 2
One of the first things to consider, regarding the function of the piriformis, is the position of the knees during something such as the overhead squat assessment. The knees demonstrating valgus during a squat assessment indicates that the piriformis isn’t holding up its end of the bargain in maintaining the femur in alignment (Fig. 3).
Since the muscle is an abductor at these angles, if the knees are adducting then the muscle is lengthening. However, most clients will still think the piriformis needs to be stretched.
Why? Because it “feels” tight. Remember that just because muscles feel a certain way doesn’t mean that they are short and need to be stretched. Muscles have an extensibility component much like a rubber band (only far more sophisticated). The more they are pulled, the tighter they get.
Therefore, if a client’s knees demonstrate the valgus position, the piriformis does NOT need to be stretched. However, if a client demonstrates knee varus (Fig. 4), then the piriformis may be short and warrant stretching.
 Fig. 3
Fig. 3
 Fig. 4
Fig. 4
Next, let us consider the muscles that are working opposite the piriformis. While there may be several, a key muscle group is the adductors. Clark, Lucett, and Sutton (2012) list the adductors as muscles that can produce hip adduction and internal rotation. Thus, the client with knee valgus may have short and overactive adductors that internally rotate the are working pull the femur and subsequently pull on the piriformis
If it has been determined that the piriformis is indeed short, then the client can proceed to stretch the muscle. First, to stretch a muscle, the opposite action needs to be performed.
The piriformis is an external rotator, so we need to set up in the internal rotation? Remember it is only a primary external rotator at neutral, and then, as the hip begins to flex, it serves more of an abduction role, until greater than 90°, then becomes an internal rotator. Thus, to perform a great piriformis stretch, the hip needs to be flexed to about a 45-65⁰ degree angle and adducted (Fig. 5) (Chaitow & Delany, 2008).
 Fig. 5
Fig. 5
 Does the performs need to be stretched? Assess to find out.
Does the performs need to be stretched? Assess to find out.
I frequently have students (who insist on stretching their piriformis differently) perform the stretch above and then quickly hear “but, I don’t feel anything.” Why do you think someone would not “feel” this stretch when performed this way? Because, they DON’T need to stretch it.
The muscle is likely long, not short. The common 90/90 piriformis stretch is valid but gets much more than the piriformis. In the position of 90° hip flexion plus the addition of external rotation, is also a great stretch for the posterior capsule of the hip. So, I could argue that many people aren’t feeling their piriformis during that stretch, but rather all the other tissues that surround the posterior aspect of the hip.
What is sciatica and what can we do about it?
Sciatica refers to pain that radiates along the path of the sciatic nerve, which branches from the lower back through the hips and buttocks and down each leg. Sciatica most commonly occurs when there is a disc herniation or lesion that compresses part of the nerve, causing inflammation, pain, and occasional numbness of the leg or part of the leg (Fig. 6) (Koes, van Tulder, & Peul, 2007).
 Fig. 6
Fig. 6
Pain originating in the lower back (or high buttock) and radiating down past the knee is a classic pattern of a true sciatica issue, meaning that is it coming from the lower back. If this is the case, the client should seek the advice of a licensed professional (DC, DO, or MD) to have the spine addressed. Foam rolling is likely NOT going to have much of an influence on true sciatica because it is originating from the spine. However, many times sciatica is confused with “Piriformis Syndrome.”
Piriformis Syndrome and what we can do about it?
Piriformis syndrome is when the sciatic nerve is not compressed by the spine but by the piriformis. This is much more of a muscular issue that may be influenced by soft-tissue work. In most individuals, the sciatic nerve runs directly through, under, or over the piriformis muscle (Fig. 7). No matter the direction, the sciatic could get compressed and become irritated.
 Fig. 7
Fig. 7
Pain originating in the buttocks or even hamstring that does NOT go below the knee could be piriformis syndrome. Usually, when this is the case, the most common treatment is to stretch the muscle. Remember from earlier, however, that stretching should only be done when the muscle is short. The over-lengthened piriformis may compress the sciatic nerve because they are contracting to attempt to pull the body back into neutral.
Receptors located in and around the muscle relay messages about the muscles position to the nervous system. If the muscle is too short, then these receptors will send a signal to relax the muscle.
Conversely, if the muscle is too long, then these receptors will send a signal to contract. Thus, muscles that are stuck in a lengthened state generally “feel” tighter than those that are short. The key is always to assess the client and to not arbitrarily stretch things.
If the problem is in fact caused by the muscle being too long then stretching would not be indicated—it is already too long. But, foam rolling would be a great way to get the muscle to calm down on a neurological level without specifically trying to add length to it.
*In most cases the piriformis is too long, not too short. Therefore, start with foam rolling and DO NOT stretch the muscle unless indicated by the movement assessment. *
Here's how to use the NASM Corrective Exercise Continuum to address the piriformis.
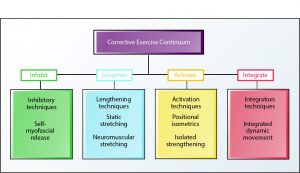 NASM Corrective Exercise Continuum
NASM Corrective Exercise Continuum
Step 1: Does the client demonstrate knee valgus (go to Step 2a) or knee varus (go to Step 2b)?
Step 2a:
- Inhibit
- Piriformis
- For the knee valgus client, use the foam roller to reduce feelings of tightness in the hip and to help mobilize all the tissues. Even the most active person stills sits more than they should, which can dehydrate all the tissues of the posterior hip. Thus, keep the leg extended and relaxed to allow more tissue displacement.

- For the knee valgus client, use the foam roller to reduce feelings of tightness in the hip and to help mobilize all the tissues. Even the most active person stills sits more than they should, which can dehydrate all the tissues of the posterior hip. Thus, keep the leg extended and relaxed to allow more tissue displacement.
- Adductors: Hold tender spots for 30-45 seconds.

- Piriformis
- Lengthen
- Adductors: 30-45 second hold

- Adductors: 30-45 second hold
- Activate
- Gluteus max: 12-20 reps

- Gluteus med: 12-20 reps

- Gluteus max: 12-20 reps
- Integrate
- Lateral tube walking: 10-15 reps each side

- Lateral tube walking: 10-15 reps each side
Step 2b:
- Inhibit
- Piriformis: Cross target leg over to “open” the hip. Hold tender spots for 30-45 seconds.

- Piriformis: Cross target leg over to “open” the hip. Hold tender spots for 30-45 seconds.
- Lengthen
- Piriformis: 30-45 second hold
- Piriformis: 30-45 second hold
- Activate
- Gluteus max: 12-20 reps
- Adductor complex

- Gluteus max: 12-20 reps
- Integrate
- Ball wall squats with a medicine ball between knees: 10-15 reps
Additional resources on corrective exercise
Stretching can be one of the most powerful tools in your personal training toolkit. But sometimes tightness doesn't necessarily mean you need to stretch.
For more information on when and how to properly stretch, as well as the scientific rationale for the discipline, check out our mini course on stretching by clicking here.
If you want to learn about fitness assessments - or you want to check out a great resource on knee biomechanics, check out the respective links!
References
Clark, M., Lucett, S., & Sutton, B. (2012). NASM essentials of corrective exercise training. Burlington, MA: Jones & Bartlett Learning.
Koes, B.W., van Tulder, M.W., & Peul, W.C. (2007). Diagnosis and treatment of sciatica. BMJ, 334(7607), 1313-1317.
Neumann, D.A. (2010). Kinesiology of the musculoskeletal system: Foundations for rehabilitation. (2nd Ed.). St. Louis, MO: Mosby Elsevier.
Reynolds, L.W., & Schrattenholzer, T.F. (2007). Piriformis syndrome. Pain Management, 2(834-836.














