Try out our free foam rolling course today and learn the importance of foam rolling!
Foam rolling is a self-myofascial release (SMR) stretching technique that has been embraced throughout the fitness industry. This effective and simple to do technique delivers positive, feel good results. Foam rollers have become easily accessible, either shared at the gym or found in almost any sporting goods aisle to bring home for a minimal investment.
Foam Rollers are also one of the go-to pieces of equipment for a Corrective Exercise Specialist or Stretching and Flexibility Coach.
Using the foam roller can deliver improvements in flexibility, muscle recovery, movement efficiency, inhibiting overactive muscles, and pain reduction with just minutes of application
Why Use Myofascial Release?
SMR can be done with a variety of tools beyond foam rollers, such as medicine balls, handheld rollers or other assistive devices. Foam rollers vary in density, surface structure, and even temperature modifications. Whatever the tool or variation selected, SMR focuses on the neural and fascial systems in the body that can be negatively influenced by poor posture, repetitive motions, or dysfunctional movements (1).
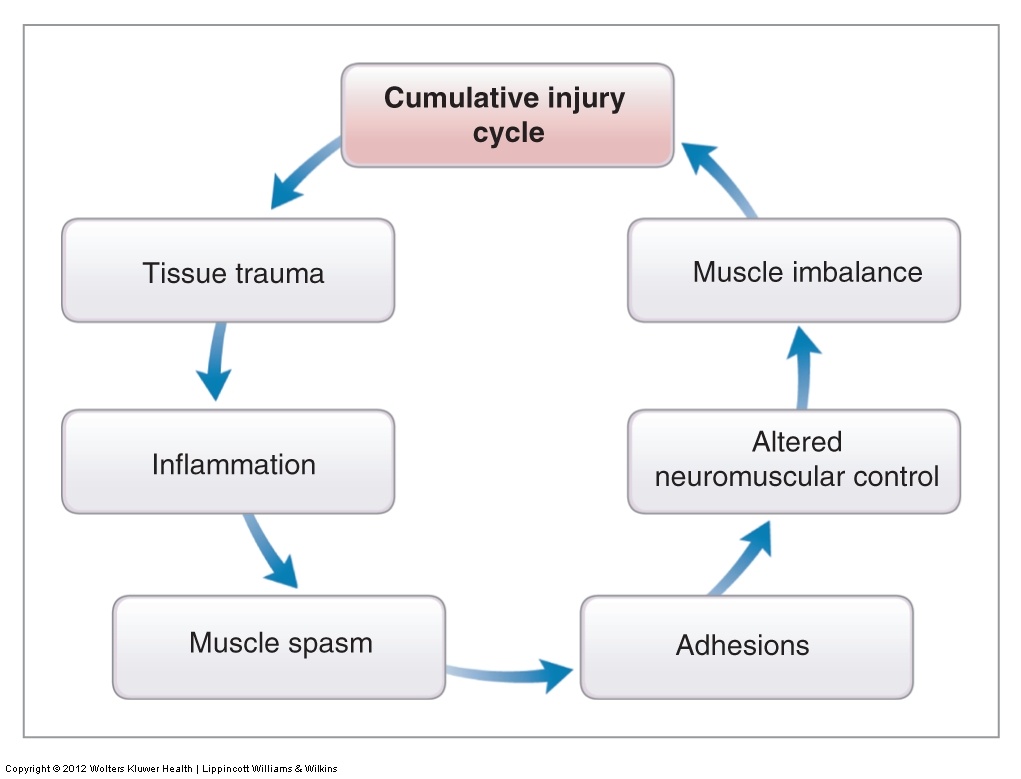
These mechanically stressful actions are recognized as an injury by the body, initiating a repair process called the Cumulative Injury Cycle (Figure 1) (1). This cycle follows a path of inflammation, muscle spasm, and the development of soft tissue adhesions that can lead to altered neuromuscular control and muscle imbalance (1-4).
The adhesions reduce the elasticity of the soft tissues and can eventually cause a permanent change in the soft tissue structure, referred to as Davis’s Law. SMR focuses on alleviating these adhesions (also known as “trigger points” or “knots”) to restore optimal muscle motion and function (1,5).
SMR is based on the principal of autogenic inhibition. Skeletal muscle tissue contains muscle spindles and Golgi tendon organs (GTO), two neural receptors. Muscle spindles are sensory receptors running parallel to muscle fibers, sensitive to a change and rate of muscle lengthening. When stimulated, they will cause a myotatic stretch reflex that causes the muscle to contract.
The GTO receptors, located in the musculotendinous junctions, are stimulated by a change and rate of tension, and when they are stimulated will cause the muscle to relax (2). When a change in tension is sustained at an adequate intensity and duration, muscle spindle activity is inhibited causing a decrease in trigger point activity, accompanied by a reduction of pain (1,6-7).
In simpler terms, when the pressure of the body against the foam roller is sustained on the trigger point, the GTO will “turn off” the muscle spindle activity allowing the muscle fibers to stretch, unknot, and realign (5).
Davis’s Law: Soft tissue models along lines of stress.
Autogenic Inhibition: The process by which neural impulses that sense tension are greater than the impulses that cause muscles to contract, providing an inhibitory effect to the muscle spindles.
The Benefits of Myofascial Release
SMR benefits include:
- Correction of muscle imbalances
- Muscle relaxation (1,2)
- Improved joint range of motion
- Improved neuromuscular efficiency (1,3,4)
- Reduced soreness and improved tissue recovery (1)
- Suppression/reduction of trigger point sensitivity and pain (2,6,7)
- Decreased neuromuscular hypertonicity (1)
- Provide optimal length-tension relationships
- Decrease the overall effects of stress on the human movement system (1)
Guidelines to Start Foam Rolling
Foam rolling should be done before static or dynamic stretching activities, improving the tissue’s ability to lengthen during stretching activities. Foam rolling can also be done as part of the cool-down (1-2). Foam rolling activities should be performed on tissues identified as overactive during the assessment process.
Most clients can enjoy foam rolling on their own once they’ve been instructed on how to properly perform the exercises. Foam rolling is not appropriate for all clients, including those with congestive heart failure, kidney failure, or any organ failure, bleeding disorders, or contagious skin conditions.
If clients have medical issues, have them seek the advice of their medical professional before starting SMR or foam rolling activities (1).
Slowly roll the targeted area until the most tender spot is found. Hold on that spot while relaxing the targeted area and discomfort is reduce, between 30 seconds and 90 seconds (1,7).
During the exercises it is important to maintain core stability. Use the drawing-in maneuver (pulling the navel in toward the spine) to maintain stability in the lumbo-pelvic-hip complex (1). Take the time to experience the exercises and discover how slightly modifying positions or angles can target different areas of the muscle.
Top Foam Roller Exercises
Here are some of the top foam roller exercises to get you and your clients started on a path to moving and feeling better.
Calves (Gastrocnemius/Soleus)

Place foam roller under the mid-calf. Cross the opposite leg over the top of the other to increase pressure. Slowly roll calf area to find the most tender spot. Hold that spot for 30-90 seconds until the discomfort is reduced. Especially beneficial for runners or those who regularly wear shoes with elevated heels (8). Switch legs and repeat.
Adductors

Lie face down and place one thigh, flexed and abducted, over the foam roller. Slowly roll the upper, inner thigh area to find the most tender spot. Hold for 30-90 seconds until the discomfort is reduced. Switch legs and repeat.
Tensor Fascia Latae (TFL)

Lie on one side with the foam roller just in front of the hip. Cross the top leg over the lower leg, placing that foot on the floor. Slowly roll from the hip joint down toward the knee to find the tender spot. Hold for 30-90 seconds until the discomfort is reduced. Switch sides and repeat.
Piriformis
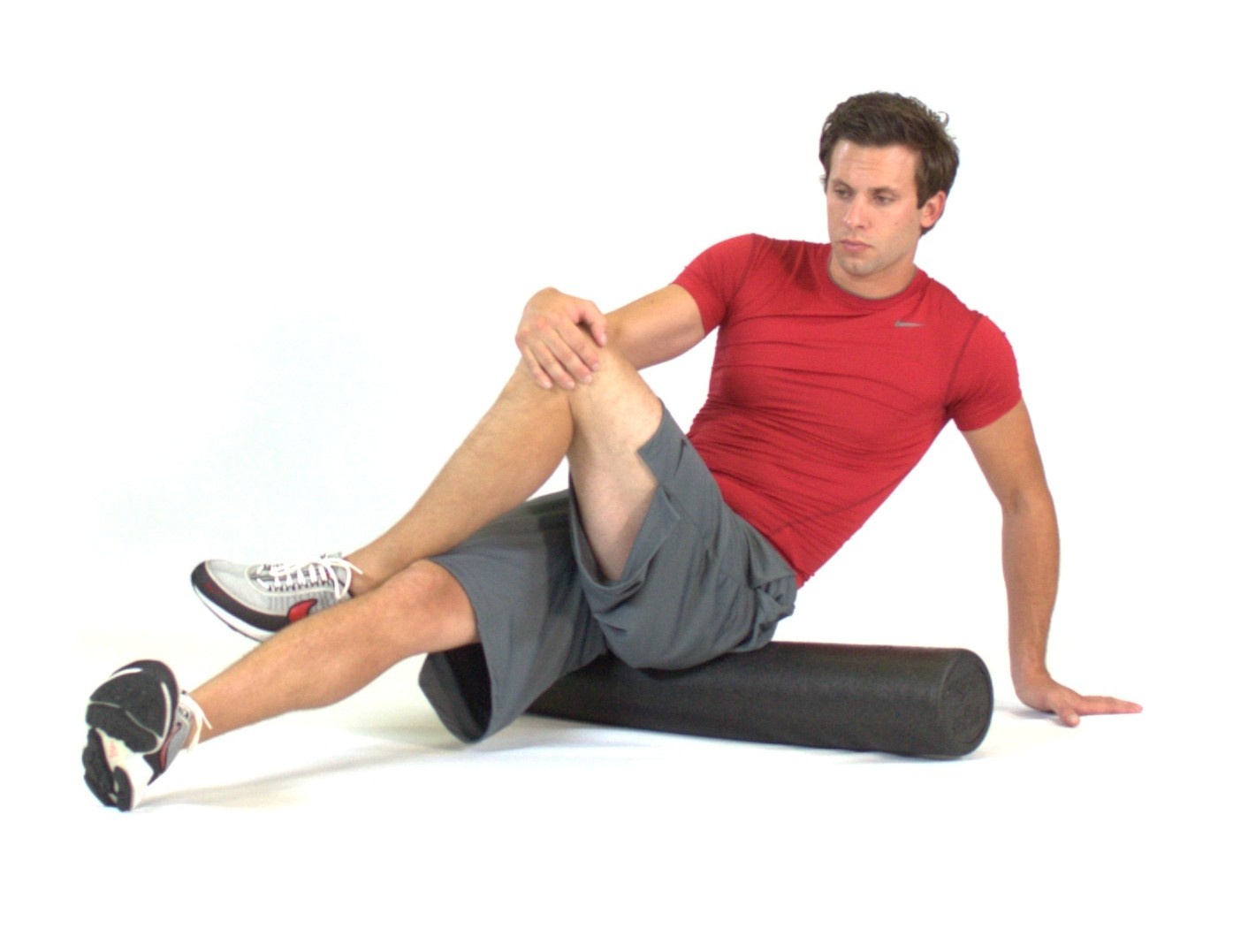
Sit on top of the foam roller, positioned on the back of the hip, crossing one foot over the opposite knee. Lean into the hip of the crossed leg. Slowly roll on the posterior hip area to find the tender spot. Hold for 30-90 seconds until the discomfort is reduced. Repeat on other side.
Latissimus Dorsi
 Lie on one side with the arm closest to the ground outstretched with thumb facing upwards. Place the foam roller under the arm in the axillary region. Slowly roll back and forth to find the tender spot. Hold for 30-90 seconds until the discomfort is reduced. Repeat on other side.
Lie on one side with the arm closest to the ground outstretched with thumb facing upwards. Place the foam roller under the arm in the axillary region. Slowly roll back and forth to find the tender spot. Hold for 30-90 seconds until the discomfort is reduced. Repeat on other side.
Thoracic Spine

Lie on the floor with the foam roller behind the upper back. Cross arms to opposite shoulders. Raise hips off the floor and slowly roll back and forth to find the tender spot. Hold for 30-90 seconds.
Just make sure you don't foam roll the lower spine!
Be sure to check out NASM's YouTube station for more SMR videos like this:
References
- Clark MA, Lucett SL. NASM Essentials of Corrective Exercise Training, Baltimore, MD:Lippincott Williams & Wilkins;2011.
- Clark MA, Lucett SL. NASM Essentials of Personal Fitness Training 4th ed. Baltimore, MD:Lippincott Williams & Wilkins;2012.
- Edgerton VR, Wolf S, Roy RR. Theoretical basis for patterning EMG amplitudes to assess muscle dysfunction. Med Sci Sports Exerc 1996;28(6):744-751.
- Janda V. Muscle weakness and inhibition in back pain syndromes. In: Grieve GP (ed). Modern Manual Therpay of the Vertebral Column. New York: Churchill Livingstone, 1986.
- Reid DA, McNair PJ. Passive force, angle and stiffness changes after stretching of hamstring muscles. Med Sci Sports Exer 2004;36(11):1944-48.
- Hanten WP, Olson SL, Butts NL, Nowicki AL. Effectiveness of a home program of ischemic pressure followed by sustained stretch for treatment of myofascial trigger points. Phys Ther 2000;80:997-1003.
- Hou CR, Tsai LC, Cheng KF, Chung KC, Hong CZ. Immediate effects of various therapeutic modalities on cervical myofascial pain and trigger-point sensitivity. Arch Phys Med Rehabil 2002;83: 1406-14.
- Grieve R, et al. The immediate effect of soleus trigger point pressure release on restricted ankle joint dorsiflexion: A pilot randomised controlled trial. J Bodyw Mov Ther.2011;15:42-49.