

Personal trainers will likely encounter a client with hip impingement as a training concern. Improve your client’s hip mobility with these stretching and strengthening techniques, plus cueing advice for pelvic positioning.
Hip discomfort or pain is common among active and sedentary adults. However, up until recently, the prevalence of hip impingement - femoroacetabular impingement (FAI) - was relatively unknown. Roling, Mathijssen, and Bloem (2016) identified only 17% of patients reporting with hip pain to be radiologically diagnosed with FAI. However, an additional 30% had “high suspicion” of FAI. Together, these statistics suggest that it may be very common among the general population. I will add that over the fifteen plus years I’ve been in the fitness industry, it seems as though the prevalence of the condition is increasing. It is likely that this is just a matter of awareness as hip mobility has become somewhat of a trend. This awareness is fortunate as a decrease in hip mobility is related to debilitating conditions, such as low back pain in certain sports (Harris-Hayes, Sahrmann, & Van Dillen, 2009). However, this incessant focus on hip mobility without an understanding of certain principles may be contributing to the prevalence of FAI.
FAI occurs when areas of bone on the acetabular rim, femoral head-neck junction, or both adversely contact and eventually damage the acetabular labrum and cartilage (Armstrong & Hubbard, 2016). This impingement occurs in the anterior aspect of the joint as the femoral head migrates forward. For comparison sake, this is no different than shoulder impingement syndrome due to the humeral head sliding anteriorly. The individual with FAI will generally report pain increasing overtime versus a one-time event that results in hip pain. Armstrong and Hubbard (2016) describe that individuals usually “place a hand over the side of the hip and report that they feel a deep pain located between their fingers and thumb; known as the C sign.” It is also common for clients to occasionally experience a catching, locking, or clicking sound.
It makes sense that FAI occurs when tissues in the iliofemoral joint are compressed and eventually damaged. However, what does not always make sense is why it happens to seemingly healthy, average individuals and among those focused on hip mobility, pelvic posture, and even hip strength. The following theories are not something I’ve generated in isolation, but are based on theories, thoughts, and anecdotal evidence I’ve attained from conferences, continuing education courses, and through numerous conversations with those much smarter and with much more experience than me. The theories are to re-think posture, stretching and mobilization techniques, and glute strengthening.
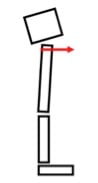 Figure 1
Figure 1
Pelvic Posture
Simply put, we must STOP repeatedly forcing a posterior pelvic rotation. The best pelvic position is neutral, not anteriorly or posteriorly rotated - even if an instructor or trainer indicated it was best for glute activation. A posterior tilt not only forces the lower lumbar vertebrae into flexion repetitively stressing the intervertebral disc but also drives the femoral head forward in the acetabulum - thus compressing the anterior portion of the acetabular labrum and cartilage (see Figure 1). While the cue of “tuck under” or sometimes “scared dog” is used because it may help increase gluteal activation, it also increases hamstrings activation (discussed later) and we must learn how to activate the glutes around a NEUTRAL pelvis. Let me reiterate that glute activation is very important, but the glutes need to contract without the pelvis moving. It is appropriate to use the cue to help a client move from an anterior tilt to neutral, but refrain from moving into a true posterior tilt.
Stretching and Hip Mobility
It is no secret that many people have tight hips. However, flexibility and mobility should be approached systematically, using assessments to help guide when, where, and what techniques should be incorporated. Short and overactive hip flexors are common culprits in the tight hip issues that plague many people. The iliofemoral joint must be placed into extension to stretch the hip flexors. One of the easiest ways to control this is to cue that “tuck under” or “scared dog” position. Now, before you start saying I’m contradicting my previous statement about pelvic posture, take note that this is just during flexibility, not during activation and strengthening techniques. Corrective flexibility will include foam rolling and static stretching, which requires the stretch be controlled and held for 30 seconds for two sets (Clark, Lucett, & Sutton, 2014). The individual will tuck the hips - posteriorly tilt - move into the FIRST point of tension and then hold. Take note that the first point of tension will be slight hip extension during a hip flexor stretch.
Where most go wrong is the lack of attention to the pelvic position. During a hip flexor stretch, if the pelvis is allowed to dip into an anterior tilt, the hip flexors will shorten. Therefore, to feel any stretch, the person usually has to move very far forward thus placing the iliofemoral joint into too much extension. In this position, the stretch felt is most likely the anterior portion of the joint capsule. Performing this on a regular basis may weaken the anterior aspect of the capsule allowing the femoral head to more easily slide forward, again compressing and eventually damaging the acetabular labrum and cartilage.
Adding to the severity of the above position is the increasingly popular technique of using mobility bands to pull the femur even more anteriorly (see picture below). We need to understand that, in the sagittal plane, most of us need the femur to move posteriorly not anteriorly given that this position is problematic. Instead, use the band to encourage a posterior slide or glide with the hip flexed, thus opening up the anterior aspect of the joint. This can be done in either supine or a quadruped position.

 Figure 2
Figure 2
Posterior Chain Activation and Strengthening
The last piece of this puzzle is activating the posterior chain; namely, the glutes and hamstrings. It is no secret that most people have underactive glutes and, in the presence of the common anterior pelvic tilt, the hamstrings are long (Clark et al., 2014). However, long hamstrings also tend to be overactive - contracting before the glutes during hip extension. While the hamstrings are important hip extensors, if they contract before the iliofemoral stabilizers, they can wreak havoc on the hip joint. The glutes and other hip rotators serve an important function of hip stabilization, which should occur before movement. Notice in figure 2, when the glutes contract, they not only produce hip extension but will also pull the femoral head posteriorly and superiorly into the back of the acetabulum. This is not only important for iliofemoral stabilization, but it also improves mechanics and saves the anterior capsular structures.
 Figure 3
Figure 3
If the hip stabilizers do not contract first, the hamstring will drive the proximal femoral head anteriorly (see Figure 3). When this happens repetitively, there will be damage to the acetabular labrum and the cartilage on the anterior aspect of the joint. Therefore, if the hamstrings tested long in an assessment, there is no need to stretch them, but foam rolling is key to help down regulate the neuronal activity of the muscles and allow the glutes to step up and take a more active role.
There are many awesome glute activation and strengthening programs available (just look on the internet, there’s hundreds). However, to ensure optimal iliofemoral mechanics during the exercise, the glutes must activate before and more than the hamstrings. Taking only one example – the glute bridge – I’m hoping you can apply the principles below to other exercises.
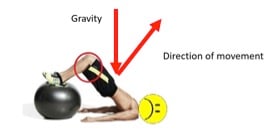
To reduce hamstring activation in a bridge, an individual must be cognizant of the direction of force, in this case gravity, and the direction of movement. To increase the level of activation of the glutes, the hips need to travel in a direction that directly opposes the direction of force. Any change in this angle will increase the activity of the surrounding musculature. Notice the angle of the tibia and the direction of movement in the picture below when the ball is placed under the feet. Since gravity is pulling the body directly towards the center of the earth, there is an increased angle between the direction of force and the direction of movement. In this exercise the hamstrings will have increased activity both because of this angle differential and the fact that they must contract to prevent the ball from rolling away.
However, notice the angles of direction of movement and direction of force in the picture with the stability ball under the shoulders and head. Here, while there may still be some hamstring contraction because they are hip extensors, there will be much less than the previous exercise.
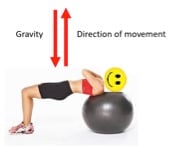
I understand that just one example may leave a lot to the imagination but think of the concept when you’re working to activate the glutes – if the exercise chosen requires more knee extension than flexion, it is likely that you’re getting more hamstring.
In summary, FAI is becoming more prevalent in all demographics. Early detection and prevention are key to help prevent or stave off more debilitating conditions such as osteoarthritis. While hip mobility and strengthening strategies are a vital part of prevention, it’s important to make educated choices on exercise selection as not all mobility and strengthening exercises are created equal.
References
Armstrong, A. D., & Hubbard, M. C. (Eds.). (2016). Hip and thigh. Essentials of musculoskeletal care (5th ed., pp. 551-639). Rosemont, IL: American Academy of Orthopaedic Surgeons.
Clark, M.A., Lucett, S.C., & Sutton, B.G. (Eds.). (2014). NASM essentials of corrective exercise training (1st Ed. Revised). Burlington, MA: Jones & Bartlett Learning.
Harris-Hayes, M., Sahrmann, S. A., & Van Dillen, L. R. (2009). Relationship between the hip and low back pain in athlete who participate in rotation-related sports. Journal of Sport Rehabilitation, 18(1), 60-75.
Roling, M. A., Mathijssen, N. M., & Bloem, R. M. (2016). Incidence of symptomatic femoroacetabular impingement in the general population: a prospective registration study. J Hip Preserv Surg, 3(3), 203-207.














