

Creating and modifying exercise programs for clients can be complicated because there are many variables to consider, including the client’s goals, tolerance for exercise, and unique physical abilities and medical history.
Moreover, there are many different exercise formats (i.e., Pilates, bodybuilding, Tabata, HIIT) fitness professionals can choose from, which can potentially cause confusion and frustration during the program design process.
It is important to note that the purpose of this article is to describe the recent updates to the OPT model rather than provide detailed teaching and full discussion of the entire model and how to use it. For those reading this article unfamiliar with the OPT Model and who wish to learn more, we recommend enrolling in the NASM's Certified Personal Trainer program. You can find special payment plan offers here.
NASM Recommendations for Program Design
To improve the program design process, NASM recommends that fitness professionals adopt an integrated approach to program design. Integrated training includes multiple forms of exercise such as flexibility; cardiorespiratory; core; balance; plyometric; speed, agility, and quickness (SAQ); and resistance training (Bennell et al., 2012; Bhagyalakshmi et al., 2007; Eriksen et al., 2002; DiStefano, DiStefano, Clark, & Padua, 2013; Ng, Sih, & Stuhmiller, 2012).
Using an integrated approach to program design can increase consistency and progression and minimize injury risk (Faude, Rommers, & Rossler, 2018; Hislop et al., 2017; Padua et al., 2018).
Keeping these concerns in mind, arguably the most crucial factor when creating an exercise program is to ensure it is adopted and adhered to by the client. Whether programs are developed for beginning exercisers, avid fitness enthusiasts, or experienced athletes, exercise programs need individuality and uniqueness to make them impactful and meaningful for clients.
These traits increase commitment and help affirm a client's success toward reaching their health, wellness, and fitness goals. These factors are the basis of NASM's Optimum Performance Training (OPT) model, its new updates, and revised guidelines.
Why NASM designed the OPT Model
NASM designed the OPT model as a planned, systematic, and periodized training program. The OPT model simultaneously improves all physical abilities, such as flexibility, muscular and aerobic endurance, core stabilization, balance, muscular strength, coordination, and power.
The OPT model is also extremely successful in helping clients and athletes from diverse populations reduce their body fat, increase lean muscle mass, and improve athletic performance and overall health. It is an evidence-based model, meaning it has been tested and validated both in a laboratory setting and with real-life clients and athletes (DiStefano et al., 2013).
The OPT includes three levels, stabilization, strength, and power, and is further subdivided into five phases (figure 1). Each phase has specific protocols, exercise guidelines, and acute variables (i.e., sets, repetitions, rest periods, etc.). These phases include:
• Phase 1 Stabilization Endurance Training.
• Phase 2 Strength Endurance Training.
• Phase 3 Hypertrophy Training*.
• Phase 4 Maximal Strength Training.
• Phase 5 Power Training.
*The name of Phase 3 is changing from Hypertrophy Training to Muscular Development Training. The name change is a better reflection of the goals of this phase. Hypertrophy, by definition, means to grow or enlarge. In the context of fitness, hypertrophy is usually referring to the enlargement of muscles. However, since hypertrophy can occur to many tissues of the body (e.g., heart, brain), NASM has decided to change the name of Phase 3 to reflect its goals better.
Figure 1- OPT Model

The OPT model should be thought of as a staircase, guiding clients through different physical adaptation levels (Table 1). This journey will involve going up and down the stairs, stopping at different steps, and moving to various heights, depending on the client’s goals, needs, and abilities.
|
Table 1 Summary Chart of the OPT Model |
|||
|
Level |
Phase |
Primary Adaptations |
Primary Methods of Progression |
|
Stabilization |
1. Stabilization Endurance Training |
· Mobility and flexibility · Core and joint stabilization · Postural alignment and control · Muscular and aerobic endurance |
· Progress exercises proprioceptively (controlled, yet unstable) · Increase the complexity of exercises once basic movement patterns have been established. |
|
Strength |
2. Strength Endurance Training |
· Core strength and joint stabilization · Muscular endurance and prime mover strength |
· Decrease rest periods. · Increase the volume of exercises (reps + sets). · Increase the load (weight) of resistance training exercises. · Increase the complexity of resistance training exercises. |
|
3. Hypertrophy Training
(Muscular Development Training) |
· Core strength · Muscular strength and hypertrophy |
· Increase the volume of exercises. · Increase the load of resistance training exercises. · Increase the complexity of resistance training exercises. |
|
|
4. Maximal Strength training |
· Core strength · Maximal muscular strength |
· Increase the load of resistance training exercises. · Increase the sets of resistance training exercises. |
|
|
Power |
5. Power Training |
· Core strength · Maximal muscular strength · Rate of force production |
· Increase the load of resistance training exercises. · Increase the speed (repetition tempo) of exercises. · Increase the sets of exercises. |
New Guidelines and Protocols for the OPT Model
At the NASM 2020 Optima Conference, new guidelines and protocols for the OPT model were revealed. These guidelines and protocols reflect the latest scientific findings and feedback from many individuals, including university professors, researchers, and practitioners, to improve client outcomes and adherence to exercise programs. New OPT guidelines reflect five primary outcomes:
1. Emphasis on training fundamental movement patterns.
2. New warm-up protocols.
3. Integrate corrective exercise.
4. Less rigidity and more creative choice.
5. Inclusion of behavior change techniques.
Training Fundamental Movement Patterns
Fundamental movement patterns are a necessity for all fitness professionals to demonstrate and teach to their clients. Fitness professionals must ensure their clients’ mastery of these movement patterns to minimize injury risk and increase exercise effectiveness.
Most exercises involve at least one of these movement patterns, though multiple movement patterns can be combined into a single exercise:
• Squatting.
• Hip hinge.
• Pulling motions.
• Pushing motions.
• Pressing.
• Multiplanar and rotational movement.
Consequently, an emphasis on training fundamental movement patterns has been added to Phase 1 of the OPT Model. Fitness professionals must master teaching, cueing, and demonstrating these movement patterns for their clients to ensure their programming safety and effectiveness.
After a client acquires basic movement proficiency (and has become accustomed to various exercise equipment), a Phase 1 program's focus shifts to improving a client’s core and joint stability and posture, similar to past protocols, this is accomplished by increasing the proprioceptive demand for exercises. In other words, exercise progressions require a greater focus on maintaining ideal postural control and balance rather than increasing external load.
A common example is a client progressing from using selectorized machines to barbells, dumbbells, and other forms of free weights. Another example includes advancing exercises from a stable seated position to a standing position or even a single-leg stance. This progression requires clients to stabilize their trunk and peripheral joints (ankles, knees, hips, and shoulders) while performing functional movement patterns. Subsequently, this creates a greater demand on the core musculature and balance mechanisms during exercise (Behm et al., 2002, 2010; Behm & Anderson, 2006; Willardson, 2007).
New Warm-up Protocols
New research has emerged regarding warm-up and stretching protocols. As a result, dynamic stretching has been added as an optional flexibility technique in all OPT model phases.
Before the new guidelines, all phases began with self-myofascial techniques (i.e., foam rolling) followed by specific stretching protocols. Traditionally, Phase 1 included self-myofascial techniques and static stretching, whereas Phases 2-4 opted for self-myofascial techniques and active stretching, and Phase 5 used self-myofascial techniques and dynamic stretching (no static or active stretching) (Table 2).
However, based on the new guidelines, fitness professionals can now include dynamic stretching in all phases of the OPT Model. Research demonstrates the benefits of dynamic stretching within a flexibility routine (Behm & Chaouachi, 2011; Behm et al., Blazevich, Kay & Mchugh, 2016; Kallerud & Gleeson, 2013; Opplert & Babault, 2018).
The addition of dynamic stretches may further increase joint range of motion while also increasing the potential expression of strength and power output. If opting to include dynamic stretching, choose one set of 3 to 10 dynamic stretches using a repetition range of 10 to 15.
|
Table 2 Warm-up Protocols |
|||
|
Level |
Phase |
Original Warm-up Protocol |
Revised Warm-up Protocol |
|
Stabilization |
Phase 1. |
· Self-myofascial Techniques · Static Stretching · Cardio (optional) |
· Self-myofascial Techniques · Static Stretching · Dynamic Stretching (optional) · Cardio (optional) |
|
Strength |
Phases 2-4 |
· Self-myofascial Techniques · Static Stretching · Cardio (optional)
|
· Self-myofascial Techniques · Static Stretching · Dynamic Stretching (optional) · Cardio (optional) |
|
Power |
Phase 5 |
· Self-myofascial Techniques · Dynamic Stretching |
· Self-myofascial Techniques · Dynamic Stretching |
Integrate Corrective Exercise Protocols
All phases in the OPT model recommend the use of core and balance exercises following the warm-up. This section of the workout is a continuation of the client’s overall warm-up. In the warm-up section, the client addressed overactive muscles by performing various flexibility techniques to improve range motion and tissue extensibility.
The next logical step is to strengthen the underactive muscles identified during the assessment process, helping reestablish ideal joint alignment, stability, and control. This can be accomplished by completing a short series of core and balance exercises. Core training is critical for improving posture (Ko & Kang, 2017; Park et al., 2016), enhancing performance (Butcher et al., 2007; Dello Iacono et al., 2016; Shinkle et al., 2012), increasing resistance to injury (Huxel Bliven & Anderson, 2013), and accelerating injury rehabilitation (Coulombe et al., 2017).
Balance training is an essential component of injury prevention programs and has been proven to help reduce the incidence of lower extremity injuries, such as ankle sprains and anterior cruciate ligament tears (Dargo et al., 2017; Nessler et al., 2017; Rivera et al., 2017). As such, core and balance training, when paired, can be a useful warm-up strategy following flexibility techniques.
However, fitness professionals knowledgeable and skilled in corrective exercise may substitute other activation techniques in this section, such as isolated strengthening techniques taught in NASM’s Corrective Exercise Specialist. Integrating isolated strengthening techniques into an OPT Model exercise program effectively combines corrective exercise and OPT.
Less Rigidity and More Creative Choice
The new updates to the OPT model include a new daily exercise template (Figure 2). A section of the new template is called Skill Development. This section is an optional portion of the workout, but it can be valuable for many clients, depending on their goals and fitness level.
The fitness professional typically assigns plyometric and speed, agility, and quickness (SAQ) exercises within this section. These forms of exercise further enhance energy expenditure and develop an individual’s agility, reaction time, and overall athleticism (Oxfeldt et al., 2019; Makhlouf et al., 2018). In addition, plyometric and SAQ training are useful modes of exercise to improve aerobic capacity and can serve as a substitute for traditional steady-state cardiorespiratory exercise, if desired.
However, fitness professionals also have the option of foregoing plyometric and SAQ exercises, choosing to substitute specialized instruction for skill acquisition. For example, instruction for specialized exercise equipment (i.e., kettlebells, battle ropes) can be included in this section of the workout template.
For more advanced clients, the fitness professional can teach new skills such as practicing MMA-inspired exercises (e.g., kicking and punching a bag), learning the intricacies of Olympic weightlifting, or integrating mind-body activities (e.g., Pilates, yoga, tai chi). It is essential to recognize that any exercises chosen in this section by the fitness professional should be specific to the client’s physical capabilities, goals, and exercise preferences.
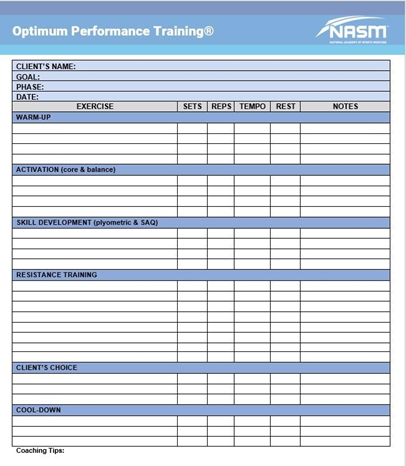
Figure 2-Daily exercise template
Inclusion of Behavior Change Techniques
Arguably the most crucial consideration when developing exercise programs is to ensure client adherence. Fitness professionals can significantly influence their client’s health, body composition, and athletic performance. Therefore, the fitness professional has a responsibility to create an environment that helps the client adhere to a fitness routine.
They should help clients feel confident and competent while preserving their autonomy to do exercises they enjoy. Self-efficacy is a well-established determinant of exercise behavior, so to promote changes that increase exercise adherence, a behavior change technique that influences self-efficacy should be used. This is the basis for the new Client’s Choice section of NASM’s daily exercise template.
In this section, the client chooses a few of their favorite exercises to include in the program. Some clients may choose to perform strength-training activities for their arms for aesthetic purposes. Other clients may opt for additional abdominal exercises or accessory lifts, depending on their likes and dislikes. Fitness professionals should encourage clients to choose a few (typically one or two) of their favorite exercises and only intervene if the desired movement is unsafe.
References
Behm, D. G., & Anderson, K. G. (2006). The role of instability with resistance training. Journal of Strength & Conditioning Research, 20(3), 716–722. https://doi.org/10.1519/00124278-200608000-00039.
Behm, D. G., Anderson, K., & Curnew, R. S. (2002). Muscle force and activation under stable and unstable conditions. Journal of Strength & Conditioning Research, 16(3), 416–422. https://doi.org/10.1519/1533-4287(2002)016<0416:mfaaus>2.0.co;2.
Behm, D. G., Blazevich, A. J., Kay, A. D., & McHugh, M. (2016). Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: A systematic review. Applied Physiology, Nutrition, and Metabolism, 41(1), 1–11. https://doi.org/10.1139/apnm-2015-0235.
Behm, D. G., & Chaouachi, A. (2011). A review of the acute effects of static and dynamic stretching on performance. European Journal of Applied Physiology, 111(11), 2633–2651. https://doi.org/10.1007/s00421-011-1879-2.
Bennell, K. L., Ahamed, Y., Bryant, C., Jull, G., Hunt, M. A., Kenardy, J., . . . Keefe, F. J. (2012). A physiotherapist-delivered integrated exercise and pain coping skills training intervention for individuals with knee osteoarthritis: A randomized controlled trial protocol. BMC Musculoskeletal Disorders, 13(129), 1–17. https://doi.org/10.1186/1471-2474-13-129.
Bhagyalakshmi, S., Nagaraja, H., Anupama, B., Ramesh, B., Prabha, A., Niranjan, M., & Shreedhara, A. (2007). Effect of supervised integrated exercise on heart rate variability in type 2 diabetes mellitus. Kardiologia Polska, 65(4), 363–368; discussion 369.
Butcher, S. J., Craven, B. R., Chilibeck, P. D., Spink, K. S., Grona, S. L., & Sprigings, E. J. (2007). The effect of trunk stability training on vertical takeoff velocity. Journal of Orthopaedic & Sports Physical Therapy, 37(5), 223–231. https://doi.org/10.2519/jospt.2007.2331.
Coulombe, B. J., Games, K. E., Neil, E. R., & Eberman, L. E. (2017). Core stability exercise versus general exercise for chronic low back pain. Journal of Athletic Training, 52(1), 71–72. https://doi.org/10.4085/1062-6050-51.11.16.
Dargo, L., Robinson, K. J., & Games, K. E. (2017). Prevention of knee and anterior cruciate ligament injuries through the use of neuromuscular and proprioceptive training: An evidence-based review. Journal of Athletic Training, 52(12), 1171–1172. https://doi.org/10.4085/1062-6050-52.12.21
Dello Iacono, A., Padulo, J., & Ayalon, M. (2016). Core stability training on lower limb balance strength. Journal of Sports Sciences, 34(7), 671–678. https://doi.org/10.1080/02640414.2015.1068437.
DiStefano, L. J., DiStefano, M. J., Frank, B. S., Clark, M. A., & Padua, D. A. (2013). Comparison of integrated and isolated training on performance measures and neuromuscular control. Journal of Strength & Conditioning Research, 27(4), 1083–1090.
Eriksen, H. R., Ihlebaek, C., Mikkelsen, A., Grønningsaeter, H., Sandal, G. M., & Ursin, H. (2002). Improving subjective health at the worksite: A randomized controlled trial of stress management training, physical exercise and an integrated health programme. Occupational Medicine, 52(7), 383–391.
Faude, O., Rommers, N., & Rӧssler, R. (2018). Exercise-based injury prevention in football. German Journal of Exercise and Sport Research, 48(2), 157–168.
Hislop, M. D., Stokes, K. A., Williams, S., McKay, C. D., England, M. E., Kemp, S. P. T., & Trewartha, G. (2017). Reducing musculoskeletal injury and concussion risk in schoolboy rugby players with a pre-activity movement control exercise programme: A cluster randomised controlled trial. British Journal of Sports Medicine, 51(15), 1140–1146. https://doi.org/10.1136/bjsports-2016-097434.
Huxel Bliven, K. C., & Anderson, B. E. (2013). Core stability training for injury prevention. Sports Health, 5(6), 514–522. https://doi.org/10.1177/1941738113481200.
Kallerud, H., & Gleeson, N. (2013). Effects of stretching on performances involving stretch-shortening cycles. Sports Medicine, 43(8), 733–750. https://doi.org/10.1007/s40279-013-0053-x.
Ko, K.-J., & Kang, S.-J. (2017). Effects of 12-week core stabilization exercise on the Cobb angle and lumbar muscle strength of adolescents with idiopathic scoliosis. Journal of Exercise Rehabilitation, 13(2), 244–249. https://doi.org/10.12965/jer.1734952.476.
Makhlouf, I., Chaouachi, A., Chaouachi, M., Ben Othman, A., Granacher, U., & Behm, D. G. (2018). Combination of agility and plyometric training provides similar training benefits as combined balance and plyometric training in young soccer players. Frontiers in Physiology, 9, 1611. https://doi.org/10.3389/fphys.2018.01611.
Nessler, T., Denney, L., & Sampley, J. (2017). ACL injury prevention: What does research tell us? Current Reviews in Musculoskeletal Medicine, 10(3), 281–288. https://doi.org/10.1007/s12178-017-9416-5.
Ng, L. J., Sih, B. L., & Stuhmiller, J. H. (2012). An integrated exercise response and muscle fatigue model for performance decrement estimates of workloads in oxygen-limiting environments. European Journal of Applied Physiology, 112(4), 1229–1249. https://doi.org/10.1007/s00421-011-2062-5.
Opplert, J., & Babault, N. (2018). Acute effects of dynamic stretching on muscle flexibility and performance: An analysis of the current literature. Sports Medicine, 48(2), 299–325. https://doi.org/10.1007/s40279-017-0797-9.
Oxfeldt, M., Overgaard, K., Hvid, L. G., & Dalgas, U. (2019). Effects of plyometric training on jumping, sprint performance, and lower body muscle strength in healthy adults: A systematic review and meta-analyses. Scandinavian Journal of Medicine and Science in Sports, 29(10), 1453–1465. https://doi.org/10.1111/sms.13487.
Padua, D. A., DiStefano, L. J., Hewett, T. E., Garrett, W. E., Marshall, S. W., Golden, G. M., . . . Sigward, S. M. (2018). National Athletic Trainers Association position statement: Prevention of anterior cruciate ligament injury. Journal of Athletic Training, 53(1), 5–19. https://doi.org/10.4085/1062-6050-99-16.
Park, Y. H., Park, Y. S., Lee, Y. T., Shin, H. S., Oh, M.-K., Hong, J., & Lee, K. Y. (2016). The effect of a core exercise program on Cobb angle and back muscle activity in male students with functional scoliosis: A prospective, randomized, parallel-group, comparative study. Journal of International Medical Research, 44(3), 728–734. https://doi.org/10.1177/0300060516639750.
Rivera, M. J., Winkelmann, Z. K., Powden, C. J., & Games, K. E. (2017). Proprioceptive training for the prevention of ankle sprains: An evidence-based review. Journal of Athletic Training, 52(11), 1065–1067. https://doi.org/10.4085/1062-6050-52.11.16.
Shinkle, J., Nesser, T. W., Demchak, T. J., & McMannus, D. M. (2012). Effect of core strength on the measure of power in the extremities. Journal of Strength & Conditioning Research, 26(2), 373–380. https://doi.org/10.1519/JSC.0b013e31822600e5.
Willardson, J. M. (2007). Core stability training: Applications to sports conditioning programs. Journal of Strength & Conditioning Research, 21(3), 979–985. https://doi.org/10.1519/r-20255.1.














