

Looking for an easy way to assess your client's current level of cardio and aerobic efficiency? Using the talk test to identify their ventilatory threshold can help do just that. Plus, learning to apply this information gives you the details needed to design their personalized metabolic cardio programming to achieve the goals they are chasing.
Part one of this two-part cardio series provided the scientific background to understanding the metabolic significance of ventilatory threshold one (VT1). In this article, we will describe a simple field test used to measure VT1, then discuss programming around this marker for overall health and fitness – built using a basic 2-zone model. We will also discuss how training with this model provides benefits to many individuals, those with weight loss goals as well as athletes seeking to improve their aerobic efficiency for performance.
Determining VT1
This protocol aims to identify VT1, the intensity at which continuous talking becomes challenging. This signals a shift in our primary utilization of fuels from fats to carbohydrates, also reflecting a loss in aerobic efficiency (i.e., ability to sustain fat utilization) (1).
The talk test is relatively simple to administer although it may require minor pre-scripting in regards to what will be said for “talking” to simplify the testing procedure. The test, explained below, incrementally increases the exercise intensity. It requires a steady-state (SS) response at each stage before assessing the talk test challenge as VT1 is an aerobic marker (aerobic measures necessitate SS responses). This SS response is the plateau effect or leveling-off of heart rate response after 15 – 45 seconds of exercise at an increased intensity (2). The test modality (e.g., bike, treadmill) and margin of workload increases are ideally determined by individual preferences and conditioning levels (less conditioned requiring smaller increments). Follow the steps provided below to assess VT1:
- Step One: Plan to complete 1 – 2 minute incremental stages. The actual stage length is best determined by the time needed to achieve a SS response. Each stage should incrementally increase by small workloads to avoid missing VT1 (e.g., ½ – 1mph speed, 1 – 2% grade or approximately 20 – 25 watts per stage).
- Step Two: Perform a light 3-minute warm-up (i.e., 3 out of 10 effort) before commencing the test.
- Step Three: Begin stage one, allowing time to attain SS. Record SS responses (e.g., HR, RPE, speed, wattage). Heart rate provides the most accurate measure of SS-response.
- Step Four: Next, ask the individual to complete a continuous bout of talking (described in part one) out loud. The recital must be continuous from either memory (e.g., prescripting), or from reading content but always consider balance and safety issues when reading. They should be able to maintain a normal conversational pace for 20 – 30 seconds. Most practitioners however, can usually identify the conversational challenge within the first 5-to-10 seconds.
- Step Five: Evaluate their challenge of talking continuously – the objective is to identify when talking becomes challenging (rather than comfortable, or difficult). This can be achieved by:
- Asking the individual to rate their challenge (i.e., easy, comfortable, challenging, difficult).
- Observing and listening to their respiratory rate and volume, and how it impacts their conversational pace and flow (i.e., smooth, continuous v. choppy and disjointed).*
- Step Six: If their talk-threshold is not reached, increase the stage intensity and repeat.
- Step Seven: Continue this process until the talk-threshold (VT1) is reached. Pending individual preferences, consider continuing one stage beyond the stage at which VT1 is estimated to validate your decision. Repeat this test within 2-to-3 days for reliability purposes and use the average workload response measured as their VT1 (e.g., HR, RPE).
* Gauging the Talk Challenge
- Easy – Comfortable – no compromise to talking; speaking in whole paragraphs, using longer sentences and words are not forced; chest does not appear to move significantly.
- Challenging – ability to only use shorter sentences where words are slightly forced, but not rushed; appearance of chest movement and mouth-breathing sound is more evident.
- Difficult – compromised talking where only very short sentences and phrases are possible; evident; words are forced and rushed; noticeable gasps for air in between words; chest moving significantly during ventilation; sound of ventilation (breathing) is clearly evident.
Individuals often mistake ‘difficult’ for ‘challenging’ – it is important to clearly differentiate the two; VT1 is associated with challenging talk (talk-threshold) whereas VT2 is associated with difficulty in speaking.
Table 1-1 provides an example of a continuous talk test performed using a treadmill with a preference for speed, which was incrementally increased every minute. After attaining SS at each stage, the individual’s HR and RPE were recorded as markers of intensity. Minute 7 represents this individual’s measure of VT1, yet the test proceeded through one more stage (minute 8) to validate the practitioner’s finding.
Table 1-1: A continuous talk test protocol example to determine VT1.
| Time | Speed | Talk Test | HR | RPE (10) |
| Warm-up: Min 1 – 3 | 4.0 mph | Easy | 117 | 3½ |
| Minute 4 | 5 mph | Easy | 125 | 4 |
| Minute 5 | 5.5 mph | Somewhat Easy | 133 | 5 |
| Minute 6 | 6.0 mph | Somewhat Easy | 138 | 6 |
| Minute 7 | 6.5 mph | Challenging | 142 | 6½ |
| Minute 8 | 7.0 mph | Difficult | 147 | 7 |
| Minute 9 – 11 | 4 mph | Cool down | 120 | 3 |
VT1 can vary between exercise modalities (e.g., treadmills, bikes) due to body orientation and the involvement of additional body parts, so consider individual exercise preferences when contemplating testing. If heart rate is used to measure VT1, also remember that it may be noticeably higher (as with any cardio test) if this test is conducted following resistance training. This is because of possible cardiovascular drift, an increase in HR attributed to reduced blood volume that accompanies the ‘muscle pump’ associated with resistance training which moves fluid (in blood) into the spaces between cells) (2).
Your Turn…
Now that you have reviewed a sample protocol to determine VT1, assess your own VT1, measuring HR preferably with a HR monitor. Map out your own protocol and achieve SS-HR at each stage before competing your own talk-test. Continue through incremental stages until you estimate VT1 as best as possible. Consider pushing yourself one additional level for validation purposes. Bear in mind that speaking out loud in a commercial facility may draw attention to yourself, so plan accordingly.
Key Benefits of VT1 Training
For individuals seeking to lose weight, they often participate in programs built around higher-intensities of exercise (e.g., high-intensity interval training- HIIT) believing this to be the best weight loss solution. But, consider these following points:
- The calories expended by most in exercise are generally smaller than anticipated and insignificant when compared to the total calories ingested or expended over a week (e.g., 275 – 300 kcal per session x3 sessions a week v. 17,514 calories and 12,446 kcal a week ingested for men and women respectively) (3). Furthermore, the ‘afterburn’ or EPOC (post-exercise oxygen consumption) that many hope for are generally much smaller than estimated. In fact, given this reality, new research and ideas now point to the remaining 16-hours spent awake in a day (non-exercise activity thermogenesis – NEAT) as the new frontier to successful weight loss (4-6). Yet, we continue to try to squeeze as many calories into an ever-shrinking allocation of time for exercise. The primary takeaway here is that we need to introduce new ideas and methodologies that increase total daily caloric expenditure all day long and stop emphasizing the small exercise session.
- Understanding key influencers of fuel utilization throughout a day is also part of these new ideas. Dietary macronutrient composition is perhaps the most influential determinant of what you burn (i.e., higher fat intakes shift fuel utilization to burning more fats throughout the day), but may not be the most healthy. The body’s adaptation to stressful events is another influencer – higher intensities shift fuel utilization towards carbohydrates, which, when coupled with some carbohydrate depletion and replenishment teaches the body to store more carbohydrates as glycogen (levels may double). For every additional gram of glycogen stored in the body, we also store an additional 2.4 – 2.7 grams of water, potentially increasing body weight. Although this represents lean mass, it may potentially offset any fat loss, which may demotivate an individual. Furthermore, this methodology also teaches the body how to utilize carbohydrates more efficiently, not just during exercise, but also throughout the day. Are these adaptations that a person exercising for weight loss really desires? Wouldn’t teaching the body to burn more fats all day long (not just in exercise) be a better solution?
How about the athlete? Let’s use the following scenario to understand this issue. Take an athlete burning 20 kcal/minute (e.g., 170 lb. @ 8.8 mph) – this intensity favors more carbohydrate utilization than fats (e.g., 80% of fuel from carbohydrates):
- 20 kcal/min with 80% from carbohydrates = 16 kcal/minute.
- 16 kcal/minute of carbohydrates = 4 g/minute or 240 g/hour.
- Over a 3-hour workout, the total carbohydrate burn rate = 720 g.
- What if the body only stores 500 g of muscle glycogen (normal quantity in many people)?
- We supplement with carbohydrate feeding – capped at 60 g/hour – a threshold value for a person of this size during exercise when our GI motility is restricted = 180 g over 3 hours.
- Notice the deficit of needing 720 g over 3-hours, but only having 680 g available (500 g + 180 g)? This deficit might potentially result in that person ‘bonking’ or ‘hitting the wall.’
So what are we to do? Ask the individual to slow down? Unlikely. What if his carbohydrate burn rate was dropped to 60% while maintaining that same exercise pace of 20 kcal/minute? How does this change his numbers and avoid glycogen depletion (now only needing 540 g over 3-hours)? Taking time to train athletes FIRST to become more aerobically efficient by building VT1 (i.e., burning more fats) is a critical off-season training strategy that will ultimately boost performance (2).
Programming with VT1
Figure 1-1 illustrates a systematic training model that begins by establishing aerobic efficiency as its foundation (for any health, fitness and performance goals), before pursuing anaerobic capacity and anaerobic power (aligned more with specific fitness or performance goals).
Figure 1-1: Systematic cardio training model
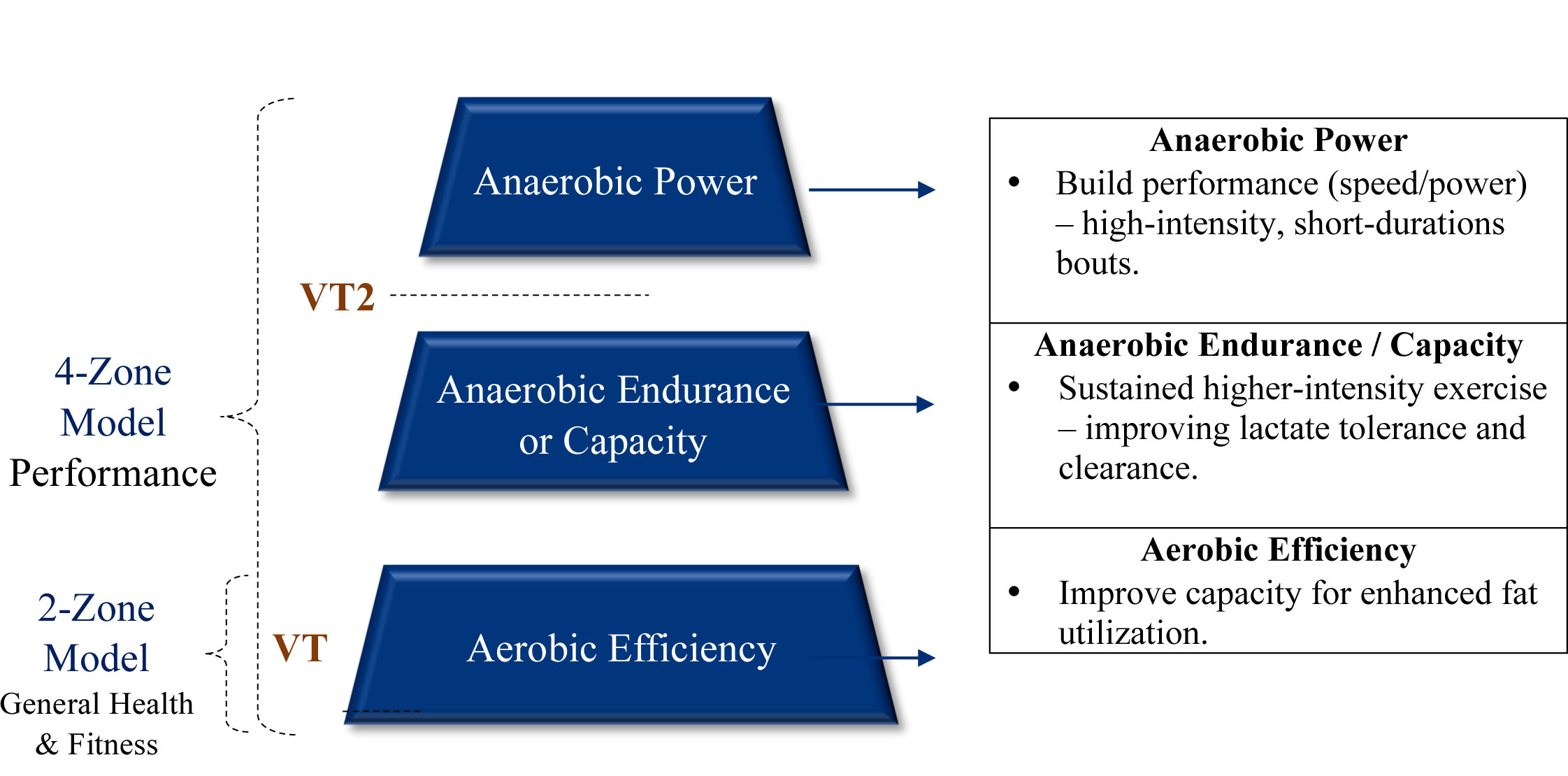
When targeting aerobic efficiency, we utilize a simple 2-zone training model:
- Zone 1 incorporates intensities below VT1-HR and is often used for recovery bouts; recovery runs following harder, longer workouts; or for programs aimed at making initial health improvements.
- Zone 2 incorporates intensities above VT1-HR where small amount of overload to the energy system (i.e., ability to keep fat as a primary fuel) build aerobic efficiency.
This 2-zone model follows four programming guidelines:
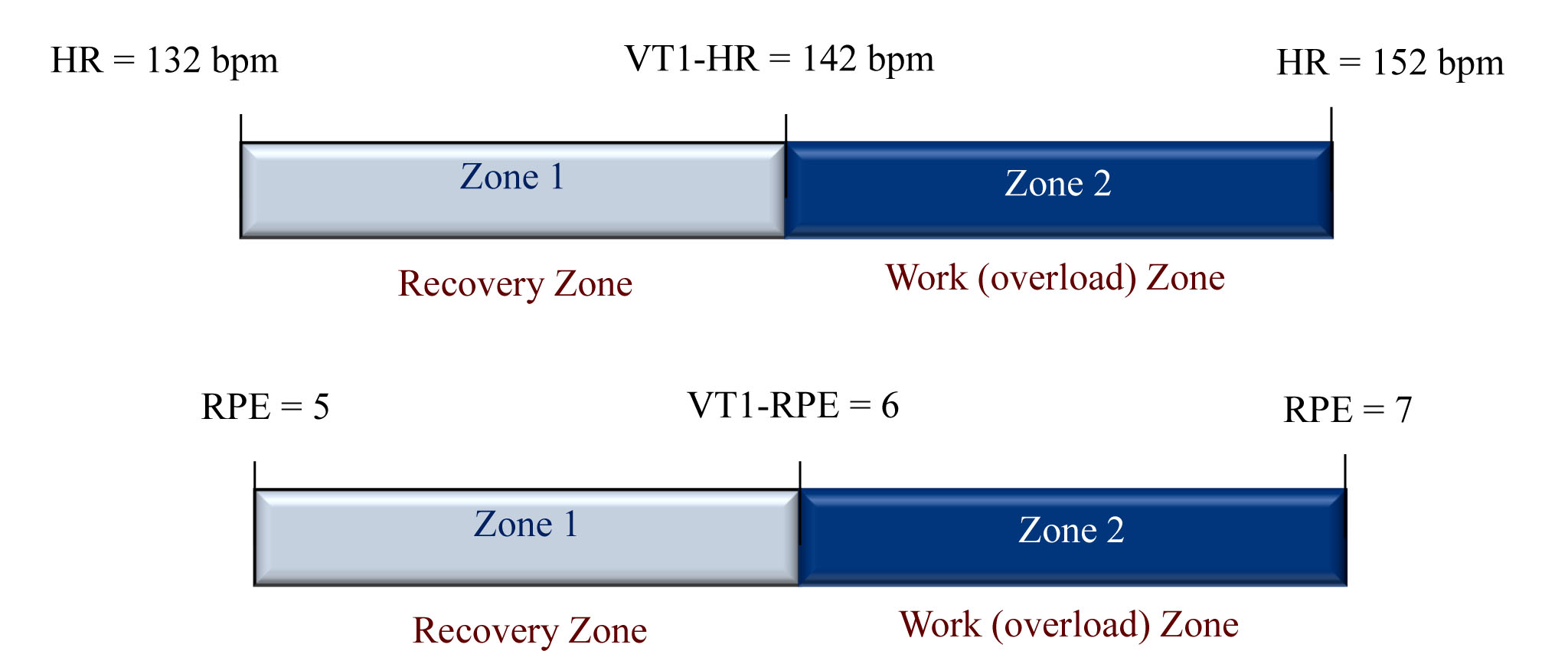
Guideline #1: Determine your zone size (smaller are better). As illustrated in Figure 1-2, zones are determined using whichever markers of intensity are measured (e.g., 10 beats defining zones, 1 mph defining zones; 1 RPE defining zones).
Figure 1-2: Using HR or RPE to determine zones.
Guideline #2: Design a 4 – 6 week training cycles as VT1 should demonstrate a noticeable shift to higher intensities (i.e., burning more calories) within 12 – 15 sessions. For example VT1-HR may move from 142 bpm to 148 bpm.
Guideline #3: Build sessions around an Aerobic Interval (AI) training format. AI format incorporates specifically-timed work intervals in zone 2, followed by specifically-timed active recoveries in zone 1. The time spent in zone 2 provides the necessary overload to enhance fat utilization at higher intensities, but this requires SS within zone 2 to be attained. Subsequently, the zone 2 workload should be no shorter than 3 minutes to ensure SS-responses plus some overload on the energy pathways. Although SS training in zone 2 (as opposed to AI) can provide adequate overload, they can often be disengaging for some and drive poorer exercise experiences.
Guideline #4: Manipulate the training variables that follow the acronym FITR. The overall goal over the 12 – 15 session microcycle is to progressively spend a greater volume of time working in zone 2 and a shorter volume of time in recovery in zone 1.
- Frequency (F): Represents the number of intervals or repetitions you plan to complete within the allotted workout time. For example, progressing from 5 x 4-minute work intervals to 6 x 4-minute bouts.
- Intensity (I): This is already defined by the zone 1 and zone 2 sizes (refer guidelines #1).
- Time (T): Represents the duration of each zone 2 work interval and also the total volume of work performed in zone 2. For example, 4 x 4-minute work intervals (total = 16 minutes) can progress to 4 x 5-minute work intervals (total = 20 minutes).
- Recovery Intervals (R): Represents the duration of the time spent in recovery between each work interval (i.e., zone 1). These are generally expressed as work-to-recovery (WTR) ratios. For example, progressing WTR from 3-to-2 to 3-to-1 indicates more time exercising in zone 2 and less time spent in recovery in zone 1 (Table 1-2).
Table 1-2: Examples of WTR Ratios when using a 4-minute work interval
| W-T-R Interval Ratio Example | Work (Zone 2) | Recovery (Zone 1) |
| 1:2 | 4 minutes > VT1-HR | 8 minutes < VT1-HR |
| 1:1 | 4 minutes > VT1-HR | 4 minutes < VT1-HR |
| 2:1 | 4 minutes > VT1-HR | 2 minutes < VT1-HR |
| 3:1 | 4 minutes > VT1-HR | 1½ minutes < VT1-HR |
| 4:1 | 4 minutes > VT1-HR | 1 minutes < VT1-HR |
After approximately 12-15 sessions, re-assess VT1 to determine whether it has moved into higher intensities. This represents improved aerobic efficiency – a greater number of calories expended each minute, but with a significant contribution being derived from fat.
In closing, as we strive to help clients achieve their unique goals, the ability to shift our programming to using markers unique to one’s individual metabolism enhances opportunities to promote better exercise experiences and attain results. Research over the past 10 – 15 years has provided such methodologies that have shifted our programming away from tools built off highly variable and flawed mathematical calculations (e.g., % maximal heart rate) towards more personalized metabolic events happening within the body. As our metabolism is as unique as our fingerprint, shouldn’t our methods for modifying metabolism be equally unique?
References:
- Persinger R, Foster C, Gibson M, Fater DC, and Pocari JP, (2004). Consistency of the talk test for exercise prescription. Medicine and Science in Sports and Exercise, 36:1612-1636.
- Pocari JP, Bryant CX and Comana F, (2015). Exercise Physiology. Philadelphia, PA., F.A. Davis and Company.
- NHANES, (2008). Trends in intake of energy and macronutrients in Adults from 1999-2000 through 2007-2008. NCHS Data Brief. Number 49, November 2010. http://www.cdc.gov/nchs/data/databriefs/db49.htm; retrieved 08/09/15.
- Katzmarzyk PT, and Lee IM, (2012). Sedentary behaviour and life expectancy in the USA: A cause-deleted life table analysis. British Medical Journal, Open, 2, e000828.
- Owen N, Sugiymama T, Eakin EE, Gardiner PA, Trembley MS, and Sallis JF, (2011). Adults' sedentary behavior determinants and interventions. American Journal of Preventive Medicine, 41:189-196.
- Katzmarzyk PT, Church TS, Craig CL and Bouchard C, (2009). Sitting time and mortality from all causes, cardiovascular disease, and cancer. Medicine and Science in Sports and Exercise, 41:998-1005.














