

Cardio programs continue to evolve given the changing needs and desires of exercisers. Driven in part by time constraints, but also by emerging research, it is the shorter, more-intense, yet time-efficient programs that are perhaps the most popular choice today. However, this format may not appeal to all, nor is it appropriate for many novice exercisers initiating exercise where positive experiences are critical to long-term adherence and success. It is more traditional steady-state (SS) or newer aerobic-interval (AI) formats that may better serve their needs. Programming recommendations do exist to guide individuals designing SS exercise, but limitations with these guidelines also exist. The focus of this article (part 1) is to discuss some of these limitations, provide a simple programming alternative for new exercisers, and then introduce the scientific principles behind what is perhaps the most accurate and personalized method for programming – one derived from specific metabolic markers unique to the individual.
Percentage of Maximal Heart Rate Error
The programming variables manipulated in designing SS programs are encapsulated by the FITT-VPP acronym (frequency, intensity, time, type, volume, pattern, progression) presented by the American College of Sports Medicine (ACSM), but hold inherent limitations (1). For example, the use of an age-predicted maximal heart rate (MHR) formula to gauge exercise intensity demonstrates significant margins of error that merit consideration in programming.
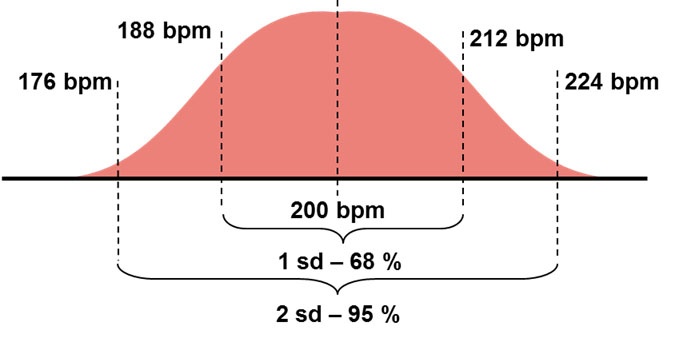
The age-predicted MHR formula, 220 – Age, continues to be used as a basis for prescribing exercise programs and as a criterion for achieving maximal exertion. Despite its widespread use as an integral part of our cardio culture for the past 45 years, its validity has been investigated and demonstrated to show significant error (2 – 5). Although this equation was originally determined arbitrarily from the results of 10 studies in the 1970s (6), subsequent research demonstrates the error in the standard deviation of this estimate to be approximately ten to twelve beats. As illustrated in Figure 1-1 and using 12 beats as an example for 20-year olds, this implies that for one standard deviation of a population (~ 68%), their true MHR falls 12 beats on either side of the calculated number, whereas for two standard deviations (~ 95% of a population), that error doubles to 24 beats. This introduces a significant error in over and under-training intensities for individuals.
Figure 1-1: The standard deviation for the 220 - Age formula using 20-year olds as an example.
Furthermore, this equation was never established with a population sample that included a sufficient number of younger and older adults. Consequently, the 220 – Age formula does not validate MHR across the entire adult age range in healthy humans. For example, a 60-year old may easily exceed a calculated MHR of 160 beats per minute (bpm) while a 20-year old may never attain 200 bpm (7). Another important consideration when using % MHR is that it fails to accommodate for discrepancies in resting heart rate (RHR) as illustrated Table 1-1. For example, an individual with a RHR of 50 bpm will need to train much harder to reach 140 bpm than an individual with a RHR of 75 bpm. This may further exaggerate the possibility of over or under-prescribing appropriate or intended training intensities for individuals.
Although this formula stipulates that people of the same age experience similar MHRs, this number varies significantly amongst people of the same age and does not show a consistent one-beat drop with age. While age explains approximately 80% of individual variances in MHR, conditioning levels and other factors also exert an influence (4). Aging does show a gradual decline in MHR due to depressed β-receptor-mediated sensitivity in the heart to catecholamines (e.g., epinephrine) and physiological changes within the sinoatrial node of the heart that lowers the heart’s inotropic (force) and chronotopic (rate) responses. The truth however, is that this number (i.e., MHR) can remain somewhat constant for 20 years in conditioned individuals (7).
Table 1-1: Discrepancy in estimating exercise intensity using %MHR between two 30-year olds.
| Person A | Person B | |
| MHR (220 – Age) | 190 bpm | 190 bpm |
| RHR | 50 bpm | 75 bpm |
| 70% MHR | 133 bpm | 133 bpm |
| Margin of Increase | 83 bpm | 58 bpm |
Other factors influence MHR – genetics exert a significant influence over both RHR and MHR that is independent of age or conditioning level. Exercise performance is not influenced by MHR and in fact, some individuals experience lowered MHRs with improved conditioning levels due to expansions in blood volume, which in turn expands stroke volume and cardiac output. MHR is also influenced by altitude where it is estimated to drop by approximately one bpm per 1,000 feet of elevation given our inability to train as hard.
Subsequently, over the past few years ACSM and other organizations have recognized that more accurate mathematical formulas for MHR exist with smaller standard deviations and now recommend that if one opts to use %MHR, to use these formulas instead of the Fox and Haskell 220 – Age calculation. Examples of some formulas are presented in Table 1-2 (1, 5).
Table 1-2: More accurate %MHR mathematical formulas
| Name | Mathematical Formula | Standard Deviation |
| Tanaka Formula | 208 – (0.7 x Age) | 7.4 bpm |
| Inbar Formula | 205.8 – (0.685 x Age) | 6.4 bpm |
| Gellish Formula | 206.9 – (0.67 x Age) | 6.6 bpm |
Your Turn: Do the Math: Using the three mathematical formulas provided in table1-2 and traditional 220-Age formula, calculate Cassidy’s and Rachel’s target heart rates at 70% MHR if Cassidy is 22 years old and Rachel is 59 years old.
A Simple Programming Alternative
Heart rate (e.g., % MHR, Heart Rate Reserve) is just one method by which we can gauge exercise intensity. Other, more simplistic methods exist like ratings of perceived exertion (RPE) and the talk-test that can improve the overall exercise experience and adherence for new exercisers.
Volume (frequency x duration) and intensity are the two primary variables manipulated in designing cardio programs and are integrated into the VIP model (volume-intensity-progression). This simple model may prove beneficial for someone starting out who is unfamiliar or ambivalent with heart rate (HR) measures or perhaps does not want to monitor HR. This model can also serve athletic individuals who favor gauging collective physiological responses rather than just heart rate. Multiplying volume by intensity provides a quantifiable number for the exerciser to target while simultaneously providing a basis for progression. The basic guidelines for using this model are to simply follow:
- Identify an appropriate frequency and duration that is manageable and attainable. For example, three times a week for 20 minutes. Multiple frequency by duration to calculate total volume (e.g., 3 x 20 minutes = 60 minutes).
- Select an appropriate intensity using an RPE score that provides the appropriate overload and experience. The table presented in Table 1-3 or the Borg 0-10 Category Ratio Scale are examples of appropriate RPE scales.
Table 1-3: Simple 1-10 RPE Scale
| Score | Description |
| 1 | I am sitting down watching TV. |
| 2 | An easy pace that I could sustain all day long. |
| 3 | A comfortable pace, but I notice a little effort. |
| 4 | I am starting to sweat, but effort is relatively easy; I can carry on a comfortable conversation. |
| 5 | It is a little above comfortable, I am sweating more, but can still talk continuously with ease. |
| 6 | The effort is becoming challenging as is my breathing; I now talk in shorter sentences. |
| 7 | I can still talk, but shorter sentences are now becoming challenging. |
| 8 | Exercise is becoming difficult as is speaking; very short sentences and phrases are possible. |
| 9 | Exercise is very difficult; only to speak a few words between breaths. |
| 10 | Exercise is extremely difficult; speaking is impossible. |
- Multiply the calculated volume by the selected intensity (e.g., 5) to determine your planned target for the week and then decide upon an appropriate progression rate (e.g., 10%). For example:
- Volume: 3 x 20 minutes = 60 minutes
- Intensity = 5-out-of-10
- Target points: 60 minutes x RPE of 5 = 300 points
Following a 10% weekly progression rate:
- Week 1 = 300 points
- Week 2 = 330 points
- Week 3 = 365 points
- Progression should be based upon achieving weekly targets, thereby earning the right to progress. While this model creates accountability in tracking individual progress, it simultaneously allows some measure of flexibility in how the targeted points can be attained as illustrated in Table 1-4. For example, the goal may be to attain the allocated weekly point total as outlined, but the model accommodates unforeseen changes that may occur in life. Options lie with manipulating the variables together (e.g., reducing workout duration, but still attaining points through frequency or intensity). Remember however, that although intensity is an efficient method to stimulate adaptation and caloric expenditure, it can also increase the likelihood of attrition associated with poor experiences. Therefore, it would make sense to define the parameters for manipulating intensity.
Table 1-4: Manipulating the programming variables
| Frequency | Duration | Intensity | Total Points |
| Planned: | |||
| 3 sessions | x 20 min | 5.0 | = 300 points |
| Variations: | |||
| 4 sessions | x 15 min | 5.0 | = 300 points |
| 2 sessions1 session | x 22 minx 16 min | 5.05.0 | = 220 points= 80 points |
| 2 sessions1 session | x 19 minx 15 min | 5.56.0 | = 209 points= 90 points |
Metabolic Markers within the Body
The traditional metabolic reference in training has long been VO2 and intensities expressed as a percentage of VO2max, VO2peak, or VO2 reserve (VO2R). Although the research supporting VO2 as a metabolic reference is strong, the practical applications of testing VO2 and monitoring intensity with it (e.g., VO2peak, VO2max, VO2reserve) limits its use. More recently, research has provided a greater understanding of metabolism and specific insight into unique ventilatory markers that we can now use in exercise programming (8). As illustrated in Figure 1-2, as exercise intensity increases, so too does ventilation in a somewhat linear fashion. Ventilatory thresholds however, describe non-linear deviations in this relationship that correspond to significant metabolic events occurring within the body called ventilatory threshold one (VT1) and ventilatory threshold two (VT2) (7). Prior to VT1, ventilation increases fairly linearly with exercise intensity, then demonstrates a slight deflection or increase (VT1). This established linear increase continues into higher intensities until a second deflection occurs, which defines VT2, an event more commonly referred to as the lactate threshold by many practitioners and the public.
Figure 1-2: Pulmonary ventilation illustrating VT1 and VT2.
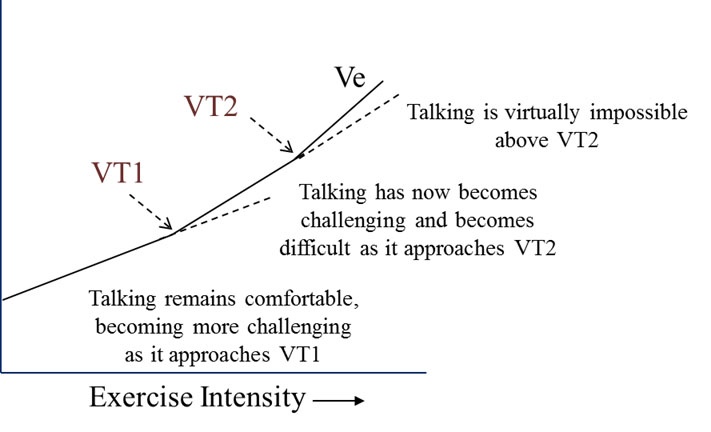
Although VT1 and VT2 can be accurately measured in a laboratory setting, estimates that can be easily measured in the field have also been developed that allow practitioners to assess these markers and program accordingly – for example, the talk test is used to measure VT1. Originally the talk test was developed as an informal, subjective method of estimating exercise intensity based upon the comfort level of engaging in continuous conversation. However, research supports the usefulness of evaluating the capacity for continuous talking as a marker for VT1. Studies conducted on various populations groups have demonstrated that the talk test is a very good marker of VT1 (9-11). One requirement for comfortable talking requires control of breath rate, but more specifically the expiration phase, which is when we talk (8). As exercise intensity progresses, ventilatory increases are attributed to expanded breath volume (defined as tidal volume), and then breath frequency.
- Below VT1, speaking in whole paragraphs and using longer sentences is generally considered comfortable. Typically, individuals will respond to a number of speech-provoking stimuli (e.g., Pledge of Allegiance, alphabet game - “A if for apple, B is for boy”, etc.) and can speak comfortably for at least 10 seconds.
- VT1 represents the point at which continuous talking is no longer comfortable (i.e., it has become challenging, but not difficult) and is generally characterized by the ability to only use shorter sentences.
- Above VT1, as one moves towards VT2, this continuous talking begins to become difficult where only very short sentences and phrases are possible. VT2 is generally identified when one can only speak a few words between breaths or when speaking is not possible.
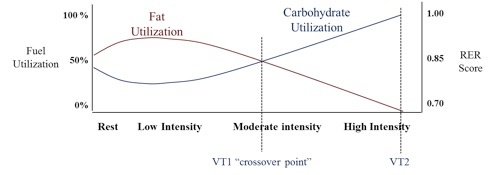
VT1 represents the exercise intensity where continuous talking moves from comfortable to becoming challenging-to-uncomfortable. As illustrated in Figure 1-3, it reflects the crossover point where our primary fuel switches from fats to carbohydrates (i.e., switching from 51% fat / 49% carbohydrate utilization to 49% fat / 51% carbohydrate utilization), which is explained in detail in the following section. But, what VT1 means as a metabolic marker is the beginning of the loss in our ability to continue utilizing fats as our primary fuel, which is a measure of aerobic efficiency or caloric quality. Effective cardio training programs, whether designed for athletes or otherwise, should never simply focus upon how hard one can work (i.e., caloric quantity). Rather, they should aim to train the body to utilize fats more efficiently during higher intensities of exercise as well as when the body is at rest.
Figure 1-3: Fuel utilization between rest and maximal exercise.
Cellular Respiration of Fuels
From a metabolic standpoint, these changes in talking represent shifting ratios of oxygen utilized and carbon dioxide produced that reflect fuel utilization that we will now explain. It is well understood that at lower intensities of exercise the body favors fat as a fuel given how the supply of oxygen is adequate to meet the additional need for metabolizing fats, and how the demand for energy is still relatively small. By examining the balanced chemical equation for a common free fatty acid used by muscle cells (i.e., palmitic acid), we notice a disparity between the quantity of oxygen used (23O2) and the quantity of carbon dioxide produced (16CO2). From this, we can deduce that the cardiorespiratory challenge to the body lies with inspiration (taking more oxygen into the body) and not with expiration where less carbon dioxide is produced that requires removal.
C16H32O2 + 23O2 = Energy + 16CO2 + 16H2O
This demand for additional oxygen under exercise stress is met initially by increasing tidal volume (TV) as evidenced by the initial changes in ventilation we witness at the onset of moderate-intensity exercise (increases in TV precede increases in breath rate). As expiration remains a slow, gradual process at these intensities – gently expelling the smaller amounts of carbon dioxide produced, it is safe to assume that a person’s ability to talk continuously should not be compromised given how talking is performed during the expiration phase. Therefore, when using the talk test, when talking remains comfortable, we can presume that fats are the primary fuel (8).
If we now examine the balanced chemical equation for glucose, presented below, we notice that the disparity in gas quantities no longer exists (i.e., between quantity of oxygen used and carbon dioxide produced). Given these equal quantities, our cardiorespiratory challenge now lies with both inspiration (inhaling more oxygen) and expiration (exhaling more carbon dioxide). Remember as well, that glucose yields less energy per molecule than a fatty acid and is favored during higher-intensity exercise. Collectively, what this means is faster utilization rates of glucose in comparison to fats and much larger volumes of oxygen needed and carbon dioxide produced.
C6H12O6 + 6O2 = Energy + 6CO2 + 6H2O
Furthermore, as we move into higher intensities of exercise, we will also begin to accumulate greater quantities of lactate and hydrogen that spill over into the blood from muscle cells given the larger contribution from our anaerobic pathways. Our need to buffer these hydrogen ions generates extra carbon dioxide which we expel from our lungs. Collectively, the more rapid production of respiratory carbon dioxide plus this additional volume derived from our buffering system creates a need for forceful expirations. A more forceful expiration shortens the duration of the expiration phase, thereby allowing the next inspiration phase to occur sooner – increasing our breath rate. As talking is performed during the expiration phase, a person’s ability to talk now becomes compromised. Breaths that are short and forced render conversation in longer sentences more challenging as they become forced and choppy. Therefore, when using the talk test, when talking becomes difficult, we can presume that glucose is the primary fuel (8).
Now that we have a clearer understanding of VT1 and talking; aerobic efficiency and fuel utilization, we can now initiate discussion on how to administer a practical field test that measures VT1, and on designing effective training programs aimed at improving aerobic efficiency. This information will be provided in Part Two of this cardio programming series.
References:
- American College of Sports Medicine, (2014). ACSM’s Guidelines for Exercise Testing and Prescription (9th). Philadelphia, PA, Wolters Kluwer/Lippincott Williams & Wilkins.
- Whaley MH, Kaminsky LA, Dwyer GB, Getchell LH, and Norton JA, (1992). Predictors of over- and underachievement of age-predicted maximal heart rate. Medicine and Science in Sports and Exercise, 24:1173-1179.
- Gellish RL, Goslin BR, Olson RE, McDonald A, Russi DG, and Moudgil VK, (2007). Longitudinal Modeling of the Relationship between age and maximal heart rate. Medicine and Science in Sports and Exercise, 39(5):822-829.
- Londeree BR, and Moeschberger ML, (1098). Effect of age and other factors on maximal heart rate. Research Quarterly for Exercise and Sport, 53:297-304.
- Tanaka H, Monahan KD, and Seals DR, (2001). Age-predicted maximal heart rate revisited. Journal of the American College of Cardiology, 37:153-156.
- Fox SM, and Haskell WL, (1970). The exercise stress test: needs for standardization. In Eliakim M, and Neufeld HN, Cardiology: Current Topics and Progress. (6th Ed). New York: Academic Press.
- Pocari JP, Bryant CX and Comana F, (2015). Exercise Physiology. Philadelphia, PA., F.A. Davis and Company.
- Persinger R, Foster C, Gibson M, Fater DC, and Pocari JP, (2004). Consistency of the talk test for exercise prescription. Medicine and Science in Sports and Exercise, 36:1612-1636.
- Ballweg J, Foster C, Pocari JP, Haible S, Aminaka N, and Mika RP, (2013). Reliability of the Talk Test as a surrogate for Ventilatory Threshold and Respiratory Compensation Thresholds. Journal of Sports Science and Medicine, 12(3):610-611.
- Quinn TJ, and Coons BA, (2011). The talk test and its relationship with the ventilatory and lactate thresholds. Journal of Sports Science. 29(11):1175-1182.
- Recalde PT, Foster C, Skempo-Arlt KM, Fater DC, Neese CA, Dodge C, and Pocari JP, (2002). The talk test as a simple marker of ventilatory threshold. South African Journal of Sports Medicine, 9:5-8.














