

Corrective Exercises are all about helping people move and feel better whether it’s while working out or just living their everyday life. In order to accomplish this, it requires a true and in-depth understanding of four phases that comprise the Corrective Exercise Continuum (CEx). These phases are:
We will cover them, and the definition of Corrective Exercise, throughout this piece.
WHAT ARE CORRECTIVE EXERCISES?
Corrective Exercises are a technique used by health & fitness professionals to address and fix movement compensations and imbalances. These exercises are commonly used by personal trainers, massage therapists and chiropractors, to help clients move and feel better both during a workout and just in their everyday life.
Within this context, the NASM Corrective Exercise Specialization teaches you how to use a variety of static and dynamic assessments to identify imbalances and use the results to design effective programs for your clients using NASM’s world-renowned Corrective Exercise Continuum.
Read more about what corrective exercise is and why it’s important.
NASM’S 4-STEP CORRECTIVE EXERCISE CONTINUUM (CEX)
The Corrective Exercise Continuum (CEx) is a simple yet highly effective four-step process fitness professionals can use with their clients and athletes to improve, and ultimately, correct common movement compensations.
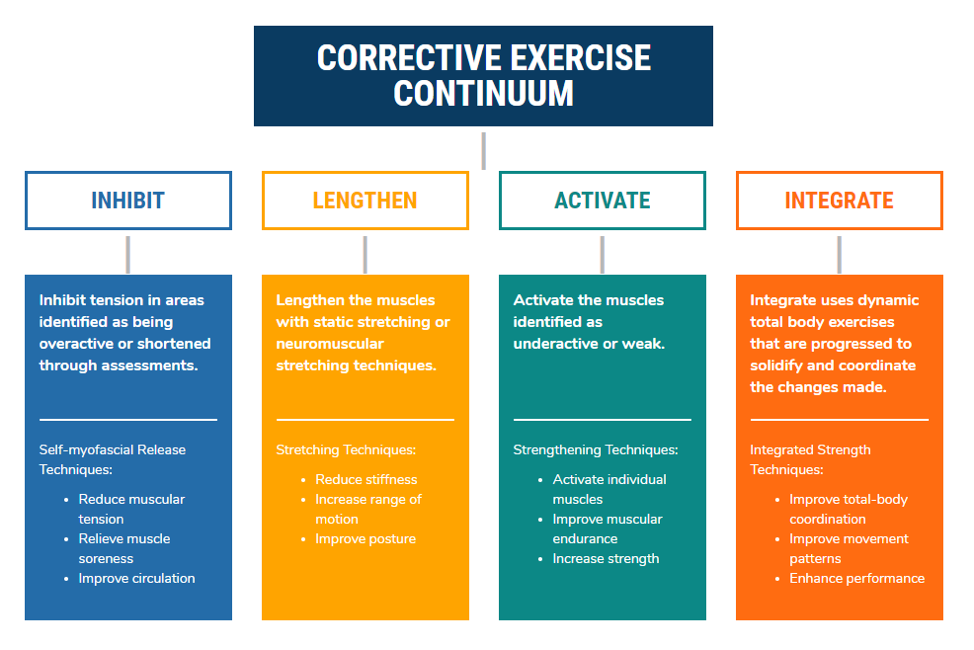
Here is a breakdown of all four steps and how best to utilize them:
CEX PHASE 1: INHIBIT OVERACTIVE MUSCLES
Inhibit is the first phase in the Corrective Exercise Continuum. The goal of the Inhibit phase is to reduce or modulate the activity of the nervous system that innervates the myofascial (Clark et al., 2014). It is essential to recognize that muscles identified as overactive (via the movement assessments) should receive inhibition techniques.
There are several corrective exercises to inhibit overactive muscles, such as foam rolling, percussion devices, or manual techniques like massage and instrument-assisted soft-tissue manipulation. However, many of these techniques require additional licensure. Thus, when it comes to corrective exercises, foam rolling is the most common for the Corrective Exercise Specialist.
The foam roller is thought to work via two primary mechanisms: 1) it affects local tissue dysfunction, and 2) it influences the autonomic nervous system (Clark et al., 2014). The ultimate goal of foam rolling is to prepare the muscle for phase 2, Lengthening, by improving local tissue mechanics and making the muscle more susceptible to stretching via afferent central nervous system (CNS) pathways (Behm & Wilke, 2018).
Research supports that foam rolling before stretching leads to enhanced improvements in flexibility and joint range of motion (Cheatham, Kolber, Cain, & Lee, 2015). These mechanisms have been further elaborated on in a series of other NASM blogs.
CEX PHASE 2: LENGTHEN (STRETCH) SHORTENED MUSCLES
Lengthening, or stretching, is the second phase in the Corrective Exercise Continuum. Contrary to popular belief, stretching does not stretch out muscle fibers. Lengthening refers to the elongation of mechanically shortened muscles and connective tissue via a nervous system response in which muscle spindle activity and motor neuron excitability are decreased (Behm, 2018).
 In other words, the muscle and connective tissue become more susceptible to forces, allowing better elongation, thus improving the range of motion. This is an essential aspect of stretching, specifically static stretching, for all fitness professionals to understand.
In other words, the muscle and connective tissue become more susceptible to forces, allowing better elongation, thus improving the range of motion. This is an essential aspect of stretching, specifically static stretching, for all fitness professionals to understand.
While stretching does have a mechanical effect, such as increasing muscle compliance, as was just noted, the real benefit of stretching is a “psycho-physiological” effect through the increased stretch tolerance (Behm, 2018). Stated more simply, static stretching will “calm a muscle down,” allowing improvement in range of motion, improved length-tension relationships, force-couple relationships, and enhanced movement patterns.
Lengthening should only be performed on those muscles which have been identified as short and overactive. A common mistake is to stretch those muscles which feel “tight.” However, due to the response of certain stretch receptors, muscles that are long are more frequently described as feeling tight than those that are short. Therefore, it is imperative that you use the findings of the movement assessments to guide the corrective exercises to build into your programming.
It may help to think of Phases 1 and 2 of the Corrective Exercise Continuum as the Mobility sections of corrective exercises. Both Inhibition and Lengthening are used before activation to improve tissue extensibility and joint range of motion before isolated strengthening. As Mennell (1964) stated, normal muscle function is dependent on normal joint movement.
For more on the scientific rationale for stretching in corrective exercise, we have a stretching mini course you can check out for free!
CEX PHASE 3: ACTIVATE UNDERACTIVE MUSCLES
The third phase of the Corrective Exercise Continuum is to Activate the underactive muscles. Activation refers to the stimulation of underactive/lengthened myofascial tissue (Clark et al., 2014). While there are a handful of activation techniques available, NASM recommends the use of isolated strengthening for Corrective Exercise Specialists.
 Isolated strengthening is a grouping of corrective exercises used to isolate specific muscles, and in some cases, to emphasize a particular part of a specific muscle, to increase intramuscular coordination and to improve force production capabilities (Clark et al., 2014). Intramuscular coordination is achieved when a muscle has optimal motor unit activation, motor unit synchronization, and the optimal firing rate (Bruhn, Kullmann, & Gollhofer, 2004; Enoka, 2015).
Isolated strengthening is a grouping of corrective exercises used to isolate specific muscles, and in some cases, to emphasize a particular part of a specific muscle, to increase intramuscular coordination and to improve force production capabilities (Clark et al., 2014). Intramuscular coordination is achieved when a muscle has optimal motor unit activation, motor unit synchronization, and the optimal firing rate (Bruhn, Kullmann, & Gollhofer, 2004; Enoka, 2015).
Similar to an intrastate highway, isolated strengthening is focused on one muscle and is not concerned with crossing over state lines into other muscles. Thus, the corrective exercises here are highly controlled and must be executed with precision.
To correctly perform these exercises, the fitness professional is encouraged to use equipment and tools necessary to help the individual to be stable and supported to focus on the specific muscle.
An example may be activation of the gluteus medius for a client that demonstrates knee valgus, indicating an underactive gluteus medius. The gluteus medius is a primary hip abductor but has anterior fibers that also produce hip flexion and medial rotation – while, on the contrary, posterior fibers produce hip extension and lateral rotation.
The client demonstrated a medial hip rotation and flexion compensation (i.e., knee valgus). Thus, the CEx Specialist needs to emphasize the posterior fibers. To do this, the CEx Specialist may have the individual also produce slight hip extension during a hip abduction exercise, thus activating the posterior fibers and middle fibers. Further, considering this, underactive core muscles are also associated with knee valgus (Shirey et al., 2012). So, the fitness professional also needs to choose a position that ensures the individual can maintain a neutral and stable spine during the gluteus medius activation exercise.
To accomplish all of what’s necessary for optimal isolated strengthening of the gluteus medius, the CEx Specialist may have the individual perform a side-lying hip abduction exercise while pressing the working leg back into a wall or stable object, often referred to as a wall slide. In this position, the client can maintain a neutral spine and target the specific fibers of the particular muscle needed to reduce the knee valgus compensation.
While not all corrective activation exercises need to be performed with a wall or lying on the ground, the fitness professional is encouraged to make sure the client always has optimal form during this phase. Use machines, tools, or any equipment necessary to help the client maintain great form.
Also, understand that this is simply a phase of training. Eventually, the training wheels will be taken off as the client becomes stronger and improves control.
For another example, check out this blog on correcting overactive hip flexors.
CEX PHASE 4: INTEGRATe WITH MULTI-JOINT MOVEMENTS
The last phase of the Corrective Exercise Continuum, Integration, is when steps 1-3 are put into action. The first three steps of the CEx Continuum have been equated to listening to individual instruments, while step 4 is listening to all the instruments playing together as a single integrated unit.
 Integration techniques are used to reteach functional movement patterns by reestablishing neuromuscular control and promoting coordinated movement (Clark et al., 2014). Integration exercises help intermuscular coordination. Like the interstate highway, these exercises do cross state lines as they use multi-joint actions and multiple muscle synergies through total-body movements.
Integration techniques are used to reteach functional movement patterns by reestablishing neuromuscular control and promoting coordinated movement (Clark et al., 2014). Integration exercises help intermuscular coordination. Like the interstate highway, these exercises do cross state lines as they use multi-joint actions and multiple muscle synergies through total-body movements.
Integration exercises are functional in that they should be movements that are important to the client, such as things they encounter daily. These exercises should begin with slow and focused movements in a controlled setting to ensure the client can maintain optimal form and control (Clark et al., 2014).
However, over time and as the client improves, the movements should be progressed by changing resistance, speed, planes of motions, base of support, introducing upper body movements, and even adding impact in some cases. Integration exercises may look and feel like the resistance training portion of Phase 1 of the Optimum Performance Training (OPT) Model.
An example of an Integrated exercise for the client with knee valgus may be a ball-wall squat with a mini-band around the knees. The squat pattern is functional, and the mini band will encourage the client to maintain proper knee position during the movement. As the client improves, the mini band may be removed (thus removing the feedback), and weights may be added to increase the resistance.
This could eventually be progressed by squatting without the use of a ball and then to changing base of support by performing a split squat or lunge. The lunge may be progressed through the three cardinal planes of motion, and finally, a squat jump may be added to enhance the eccentric demand.
Focusing on the eccentric portion of all Integration exercises and improving postural control in all planes of motion may help to reduce specific injuries (Boling & Padua, 2013). Like the Activation phase, optimal form is vital during the Integration exercises.
SUMMARY: THE IMPORTANCE OF CORRECTIVE EXERCISE
The goal of corrective exercises are to reteach a better movement pattern. This is applied to all clients, not just those recovering from injury. Thus, it is vital to follow the process of identifying movement dysfunction, following the four-phase Corrective Exercise Continuum, and to execute that program with optimal form and control.
A CEx program may serve as an intelligent warm-up or as a full 45-60 minute training session, depending on the needs of each client. Furthermore, recognizing that the last phase, Integration, works seamlessly with the Stabilization Endurance phase of the OPT Model, a CEx program can lead directly into a traditional training session. Want to learn more about Corrective Exercise? Become an NASM Corrective Exercise Specialist!














