

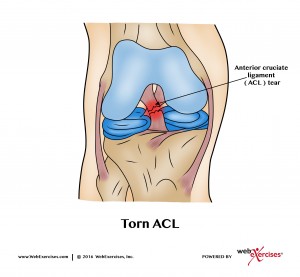
Anterior cruciate ligament (ACL) injuries are one of the most common among young female athletes occurring at a conservative estimate of 38,000 incidences per year. (1) With the cost of a surgical repair ranging between $17,000-$25,000 (2), the economic impact is significant, not to mention the long term sequela to the athlete which includes a significantly greater risk of osteoarthritis in the future. (3) Approximately 80% of these injuries are non-contact, suggesting many of them can be prevented. (4)
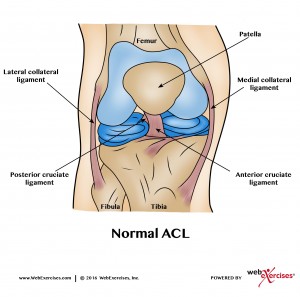
The ACL is a ligament running from the posterior femur anteriorly to the tibia. It originates from deep within the notch of the distal femur and its proximal fibers fan out along the medial wall of the lateral femoral condyle. The ACL attaches in front of the intercondyloid eminence of the tibia and is blended with the anterior horn of the medial meniscus. It provides approximately 85% of the restraining forces preventing anterior tibial translation. It also limits excessive internal or external rotation of the tibia. (5)
Pubertal females are four to six time more likely to sustain an ACL injury compared to males, thereby representing the largest demographic of athletes at potential risk. (6) This is due to a variety of reasons including the rapid growth of the femur and tibia that generate larger joint forces making neuromuscular control of the lower extremities and trunk much harder. A lack of core stability has also been shown to influence knee injuries in female athletes as reported by Zazulak and colleagues. They demonstrated this decrease in core neuromuscular control increases uncontrolled trunk displacement leading to higher knee ligament strain and ACL injury. (7)
See also: Knee Strength for Females
In order to identify at risk athletes, implementing a screening method such as the Landing Error Scoring System (LESS) test or Tuck Jump test is essential when working with all athletes in this age range. The LESS involves having the athlete stand on a 12-inch box and then jumping forward with both feet to a predetermined line followed by an immediate jump for maximal height.
The Tuck Jump test requires the athlete to perform repeated jumps flexing the knees toward the trunk for a duration of 10 seconds. Both tests have been validated in the literature to identify neuromuscular imbalances. (9) (10) (For more information on each test please refer to NASM Essentials of Corrective Exercise Training for a detailed review. (8))
One of the most common muscular imbalances identified in females over males is increased knee valgus and coronal plane rotation that has been shown to be a predictor of injury. This common finding has been associated with increased quadriceps firing and decreased gluteal activation in females, causing anterior shear stress on the tibia, which is then transferred to the ACL. (11)

In order to establish proper gluteus maximus activation, a hip bridge with a resistance band above the knees is recommended. Choi and colleagues found that gluteus maximus EMG activity was significantly greater while anterior pelvic tilt angle was significantly lower in the hip bridge with isometric hip abduction compared to the hip bridge without the band. Therefore, they concluded that performing hip bridges with isometric hip abduction against isometric elastic resistance can be used to increase gluteus maximus EMG activity and reduce anterior pelvic tilt during the exercise. (16)


Hip Bridge with Resistance Band - Begin by lying on the floor with knees bent and feet flat on the floor. Place a resistance band around the thighs just above the knees. Slightly abduct the legs while simultaneously performing a hip bridge. Slowly lower to start position without bringing knees together. Perform 3 sets of 10 repetitions.
Valgus collapse of the knee can also be associated with weakness of the hip external rotators and gluteus maximus. Paterno and colleagues identified this finding as an eight times greater risk of sustaining a second ACL injury. (12) Performing the clam shell exercise will mitigate hip rotator weakness, helping to minimize this potential risk.


Clam Shell with Resistance Band - Begin by lying on the side with knees together and bent to 90 degrees with resistance band around knees. Lift top knee upward while keeping feet touching. Continue lifting knee to the point just before pelvis begins to move. Perform 3 sets of 10 repetitions.
The hamstrings are also synergistic to the knee helping to stabilize the tibia against the anterior forces created by the quadriceps. A stability ball leg curl is a great open kinetic chain exercise and has been showed to elicit high EMG activity of the hamstring muscles while co-contracting the core musculature. (13)

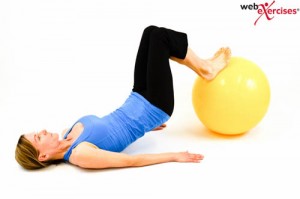
Stability Ball Leg Curl - Begin lying face up with arms extended at sides and ankles on top of the stability ball. Activate core and form a bridge position. Then flex knees, bending legs as you draw the ball inward. Reverse the movement, extending knees, and return to start position. Perform 3 sets of 10 repetitions.
In order to establish lateral stability, the side step “monster walk” with knees bent is a functional and effective exercise. Increased hip abduction strength has been shown to improve the ability of female athletes to control lower extremity alignment. (14) When performing this exercise, the stepping motion should be performed in a squat position rather than an upright straight leg position in order to generate greater gluteus maximus and medius muscle activity. (15)

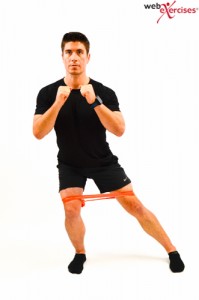
1/4 Squat with Lateral Steps Using Resistance Band - Begin standing with a resistance band around the thighs just above the knees. Keep your feet and knees apart enough to put resistance on the band. Perform a ¼ squat with both feet supporting body weight. Hold squat position, shift weight fully onto one leg. Take a lateral step with the other un-weighted leg. Repeat, taking several lateral steps in one direction and then doing the same in the other direction.
Another potential risk of injury occurs when landing with a knee flexion angle of less than 45 degrees. Therefore, performing long jumps can be used to train proper landing patterns. This exercise is similar to the Tuck Jump test with the addition of forward motion and is also a great way to introduce plyometric exercises. If the athlete is unable to “stick” the landing with toes straight ahead and no inward knee motion, then regress them to submaximal jumps of a shorter distance until perfect technique can be attainted. (6)


Long Jump to Backward Hop - Begin in quarter squat position. Jump forward in an explosive long jump trying to “stick” the landing for 3-5 seconds. Make sure the knees are flexed to approximately 90 degrees on landing. Hop backwards two or three times returning to the start position. Perform 3 sets of 10 repetitions.
One of the most significant findings, which has been shown to reduce the incidence of ACL injuries in a number of studies, is the incorporation of high-intensity plyometric exercises as part of the training program. The split jump offers these plyometric benefits.


Split Jumps - Begin in a split stance lunge position with arms raised at shoulder level. Jump upward and quickly reposition legs and land with feet in opposite positions. Raise arms while you are jumping. Continue jumps by alternating leg positions. Perform 3 sets of 10 repetitions.
If an athlete fatigues to the point that she can no longer perform the exercise perfectly, then she should be instructed to stop. The duration of each completed exercise should be noted with the goal of the next training session to continue to improve technique and to increase volume or intensity.
In addition to the NASM corrective exercise continuum of inhibit, lengthen, activate and integrate, three additional components should also be considered as part of a comprehensive training protocol. These are biomechanically correct movement patterns as noted above; neuromuscular patterning based on the identification of underlying neuromuscular imbalances as found in the assessment test; and constant biomechanical assessment through the LESS, Tuck Jump or similar test with feedback and verbal cueing to athlete both during and after training. (10)
An incorporation of a core stabilization program is not only integral but also essential in order to provide dynamic stability for the lower extremities. A weak core results in energy leakage as described by McGill requiring the weaker joints to make up for this difference. An example of this is when jumping or changing running direction, the lower extremity musculature must compensate for the lack of core stability, negatively effecting performance. (17)
All of the above displayed exercises are easy to execute and include minimal risks if performed as described. To achieve satisfying results, it is important do them on a regular basis and for a minimum of 4 weeks. The general guideline for progressing student athletes is the “10% rule”, where total training (intensity, frequency, duration, or any combination) is not increased more than 10% per week. Although there are many approaches to knee strengthening, hopefully this has provided insight into some basic strengthening strategies. Should your client’s condition worsen at any time, an evaluation with a medical professional would be warranted.
References
1) Toth AP, Cordasco FA. Anterior cruciate ligament injuries in the female athlete. J Gend Specif Med. 2001; 4:25–34.
2) de Loes, M, et al. A 7-year study on risks and costs of knee injuries in male and female youth participants in 12 sports. Scand J Med Sci Sports. 2000;10(2):90-97.
3) Ruiz AL, Kelly M, Nutton RW. Arthroscopic ACL reconstruction: a 5-9 year follow up. Knee. 2002;9(3):197-200.
4) Sadoghi, P, et al. 2012. Effectiveness of Anterior Cruciate Ligament Injury Prevention Training Programs. J Bone Joint Surg Am. 2012; 94:1-8.
5) Lowe, R. Anterior Cruciate Ligament (ACL). Retrieved from: http://www.physio-pedia.com/Anterior_Cruciate_Ligament_(ACL)
6) Myer, G. 2004. Rationale and Clinical Techniques for Anterior Cruciate Ligament Injury Prevention Among Female Athletes. Journal of Athletic Training 2004;39(4):352–364.
7) Zazulak BT, Hewett TE, Reeves NP, et al. The effects of core proprioception on knee injury: a prospective biomechanical–epidemiological study. Am J Sports Med 2007;35(3):368–73.
8) Clark, MA, Lucett, SC. (2014). NASM Essentials of Corrective Exercise Training. Burlington, MA. Jones & Bartlett Learning.
9) Padua, D. et al. 2011. Journal of Sport Rehabilitation. 20, 145-156.
10) Myer, et al. 2008. Tuck Jump Assessment for Reducing Anterior Cruciate Ligament Injury Risk. Athl Ther Today. 2008 September 1; 13(5): 39–44.
11) Zazulak, B, et al. Gender Comparison of Hip Muscle Activity During Single-Leg Landing. Journal of Orthopaedic & Sports Physical Therapy.
12) Paterno, M, et al. Biomechanical Measures During Landing and Postural Stability Predict Second Anterior Cruciate Ligament Injury After Anterior Cruciate Ligament Reconstruction and Return to Sport. Am J Sports Med October 2010 vol. 38 no. 10 1968-1978.
13) Panagiotis, T., et al. 2015. Muscle and intensity based hamstring exercise classification in elite female track and field athletes: implications for exercise selection during rehabilitation. Open Access Journal of Sports Medicine. 6:209-217.
14) Myer , G, et al. 2008. Trunk and Hip Control Neuromuscular Training for the Prevention of Knee Joint Injury. Clin Sports Med 27:425–448.
15) Berry, et al. 2015. Resisted side-stepping: the effect of posture on hip abductor muscle activation. Journal of Orthopaedic & Sports Physical Therapy.
(16) Choi, C, et al. 2014. Isometric hip abduction using a Thera-band alters gluteus maximus muscle activity and the anterior pelvic tilt angle during bridging exercise. Journal of Electromyography and Kinesiology.
(17) McGill, S. Core Training: Evidence Translating to Better Performance and Injury Prevention. Strength and Conditioning Journal. Vol 32(3):33-46.
(18) Myer, G. 2006. The effects of plyometric vs dynamic stabilization and balance training on power, balance, and landing force in female athletes. Journal of Strength and Conditioning Research. 20(2), 345-353.














