

Plantar fasciitis is the most common cause of heel pain, responsible for approximately 2 million orthopedic office visits annually and reported to affect between 10 and 20% of injured athletes. (1, 2) It affects males more often than females between the ages of 40 and 60, partly due to degeneration of the calcaneus fat pad after the age of 40. (3) Plantar fasciitis can be characterized by pain in the heel when weight bearing and is generally worse in the morning when taking the first steps out of bed and with prolonged inactivity. (4) This pain can limit activity and ultimately affect the fitness goals of your clients.
Risk factors include running, prolonged weight bearing, obesity, and limited ankle dorsiflexion, all of which are commonly seen with personal training clients. However, in order to understand how to incorporate corrective exercise we must first look at the foot anatomy and how the plantar fascia functions and works as part of the normal gait cycle.
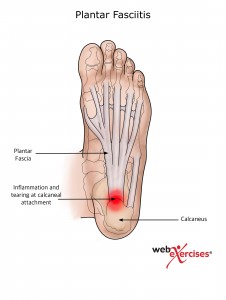
To begin with, the plantar fascia forms a mechanical linkage between the calcaneus and the toes. It originates at the calcaneus and spreads broadly as it extends into five bands inserting into the base of each proximal phalanx. (5) The plantar fascia is influenced by several factors including arches that are too low resulting in too much motion or high arches resulting in too little motion. (6) During normal gait the great toe should dorsiflex properly thereby tightening the plantar fascia and shortening the distance between the calcaneus and metatarsals. This action is known as the windlass mechanism principle. (7) Any alteration in the mechanism will lead to compensation and breakdown of normal biomechanics.
Prolonged weight bearing activities as noted above can cause posterior tibialis weakness and plantar fascia elongation. (8) This is problematic as the posterior tibialis is responsible for eccentrically controlling pronation, therefore, strengthening this muscle should be included as part of an exercise programming plan.
In addition to the ankle and foot assessments found in NASM Essentials of Corrective Exercise Training, limited dorsiflexion may be the most important predictor of plantar fasciitis when compared to obesity and prolonged weight bearing. One potential cause of this may be related to a shortened Achilles tendon. This results in excessive pronation to compensate for the lack of motion, thus putting excessive stress on the plantar fascia. (3) Normal dorsiflexion is 20 to 24 degrees so it is important to assess how much mobility your clients have. (10)
Ankle Dorsiflexion Assessment
A simple way to assess this is to have your clients begin in a half kneeling position with a dowel perpendicular to the floor, four inches in front of the their great toe. Have them glide forward keeping their heel firmly on the floor and measure how close their knee comes to the dowel. Repeat on the opposite side to compare the results. Once dorsiflexion has been assessed, an intervention strategy can be implemented for the plantar fascia, calf and posterior chain muscles.


Following the NASM corrective exercise protocol of inhibiting and lengthening muscles is an effective starting point to allow for proper great toe dorsiflexion to occur in the windlass mechanism. Stretching the calf and plantar fascia are also regularly suggested as an intervention, as seen by DiGiovanni and colleagues. They compared a standing Achilles tendon stretch (Figure A) to the seated plantar fascia stretch (Figure B). Their findings indicate plantar fascia stretching produced superior results with regards to pain, function and overall satisfaction. (9)
 Figure A
Figure A
 Figure B
Figure B
Plantar Fascia Stretch (Figure B) - To perform the plantar fascia stretch, begin in a seated position with the foot placed on the opposite knee. Place thumb alongside ball of foot and grasp first metatarsal (first toe) with remaining fingers. Extend until stretch is felt under the ball of the foot. Hold for 10 seconds and repeat 10 times. Perform this 3 times per day. (9)
Next, integrate stretching of the posterior chain. Several studies have suggested posterior muscle tightness could be involved in the etiology of plantar fasciitis. (13) Therefore a combination of self-myofascial release (SMR) to both the plantar fascia and posterior chain muscles, as suggested by Mohr and colleagues, is recommended. They compared hamstring stretching to foam rolling prior to stretching and found that in order to maximize gains in flexibility foam rolling should be performed in combination and prior to stretching. (11)
Hamstring Foam Rolling - Begin seated on the floor, legs extended with foam roll under the hamstrings. Hands should be placed at sides, supporting the body. Cross one leg over the other and lift hips off of the floor. Gently move foam roll throughout hamstrings, as tolerated, maintaining consistent pressure with foam roll. Perform three 1 minute repetitions with 30 second breaks in order to rest your arms.

Adding SMR to the plantar fascia has also been suggested to enhance the flexibility of the posterior chain as reported by Grieve et al. They studied the effects of performing two repetitions of two minute bouts of tennis ball rolling on the plantar fascia of each foot, from the metatarsal heads to the heel, focusing on the medial arch. They concluded that a single session of bilateral SMR led to increased hamstring and lumbar flexibility. (12)
Plantar Fascia SMR - Begin standing barefoot with the tennis ball underneath the arch of the foot. Slowly roll back and forth, massaging the plantar surface of the foot while maintaining consistent pressure with the ball. Perform three 1 minute repetitions with a 30 second break between bouts.


In order to activate the weakened tibialis posterior muscle that occurs with prolonged weight bearing as noted above, an ankle inversion exercise using a resistance band is suggested. (7)
Ankle Inversion with Resistance - Begin seated in a chair. Place resistance band around forefoot, anchoring the opposite end to a firm structure. Maintain alignment between kneecap and second toe with knee bent to 90 degrees. Lift forefoot off the floor and invert ankle in a scooping motion against resistance band. Slowly return to starting position. Perform 3 sets of 10 repetitions focusing on eccentric control.


In addition to the tibialis posterior, a plantar flexion exercise is also suggested. This can be done by performing heel raises with the foot in a toe-in position.
Toe-In Heel Raise - Begin standing with feet pointed inward so that the toes are close together. Lift heels off the floor. Pause momentarily then slowly return to start position. Perform 3 sets of 10 repetitions.


Proximal muscle weakness, including the gluteus medius, tensor fascia latae or quadriceps, can contribute to plantar fasciitis as well. This weakness can lead to poor shock absorption resulting in greater transmission of forces to the foot structures. (7) Therefore, a comprehensive program will address both stretching and strengthening of the local and global muscles.
Considerations for exercise programming to improve plantar fasciitis.
It is of utmost importance that clients with existing plantar fasciitis pain be cleared by their physician before starting an exercise program. If the client has completed physical therapy, you can use the exercises that they have learned during their sessions as a good starting point and base for progression or refer to NASM Essentials of Corrective Exercise Training for additional recommendations.
Here are some general guidelines for working with clients with previous or existing musculoskeletal conditions (14):
- Never exercise through pain.
- Groove appropriate and perfect motion and motor patterns before adding load or other challenges.
- Start by taking gravity out of the equation; start supine or prone, quadruped, kneeling, then standing.
- Increase intensity or time, but not both.
- Intensity can be increased by either changing resistance or changing stability.
If the client is ready to be progressed, the following guidelines will help you do this safely and effectively (15):
- If the client is still making progress then continue with the current workload.
- If the client is at a plateau then progress at a 2-10% increase.
- If the patient experiences a flare-up then decrease volume.
Download the plantar fasciitis exercise program here.
References
- Riddle, D., Schappert, S. 2004. Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: a national study of medical doctors. Foot Ankle Int. 25(5):303-10.
- Taunton, J., et. al. 2002. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 36:95–101.
- Riddle, D., et al. 2003. Risk Factors for Plantar Fasciitis: A Matched Case-Control Study. The Journal of Bone and Joint Surgery. 85-A(5):872-877.
- Cole, C., et. al. 2005. Plantar Fasciitis: Evidence-Based Review of Diagnosis and Therapy. Am Fam Physician. 72:2237-42, 2247-8
- Neufeld, S., Cerranto, R. 2008. Plantar Fasciitis: Evaluation and Treatment. J Am Acad Orthop Surg. 16:338- 346.
- Tiberio, D. 1988. Pathomechanics of Structural Foot Deformities. Physical Therapy. 68(12):1840-1849.
- Bolgla, L., Malone, T. 2004. Plantar Fasciitis and the Windlass Mechanism: A Biomechanical Link to Clinical Practice. Journal of Athletic Training. 39(1):77–82.
- Thordarson, B. et al. 1995. Dynamic support of the human longitudinal arch: a biomechanical evaluation. Clin Orthop. 316:165–172.
- DiGiovanni, B., et al. 2006. Plantar Fascia-Specific Stretching Exercise Improves Outomes in Patients with Chronic Plantar Fasciitis. The Journal of Bone and Joint Surgery. 88-A(8):1775-1781.
- Ekstrand, J., et al. Lower extremity goniometric measurements: A study to determine their reliability. Arch Phys Med Rehab 1982; 63:171-175.
- Mohr, A., et al. 2014. Effect of Foam Rolling and Static Stretching on Passive Hip-Flexion Range of Motion. Journal of Sport Rehabilitation. 23:296-299.
- Grieve, R., et al. 2015. The immediate effect of bilateral self myofascial release on the plantar surface of the feet on hamstring and lumbar spine flexibility: A pilot randomised controlled trial. Journal of Bodywork and Movement Therapies. 19(3):544-52.
- Bolivar, Y., et al. 2013. Relationship Between Tightness of the Posterior Muscles of the Lower Limb and Plantar Fasciitis. Foot & Ankle International. 34(1):42–48 .
- Adapted from Ed LeCara, PhD, DC, MBA, ATC, CSCS.
- Med Sci Sports Exerc. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. 2009 Mar; 41(3):687-708.














