


Creatine monohydrate is currently the most effective performance enhancement supplement for persons seeking to improve their high-intensity exercise capacity (i.e., acute performance enhancement including the quality of each training session and production on game/competition day), and/or increase exercise-induced lean body mass (LBM). But what does creatine really do?
The goal of creatine monohydrate supplementation (CS) is to deliver a greater and prolonged accrual of gains, as opposed to a non-supplemented state, that can translate to the “field of play” (specific sport activities) because continuous better workouts allow greater and continuous improved muscular adaptations. Moreover, the safety of CS is undisputed, and in fact offers therapeutic and recovery benefits in otherwise healthy individuals of all ages.
What is Creatine, how much is naturally in the body, and why would I supplement
A naturally occurring energy compound that supplementation can increase to improve performance.
Creatine (Cr) is a naturally occurring amino compound found in skeletal, cardiac, smooth muscle, and brain that plays an indispensable role in energy metabolism in almost all tissues.[i] The body produces creatine from the amino acids methionine, glycine, and arginine (folate and vitamin B 12 are also catalysts), with most residing in skeletal muscle (SM) where about one-third exists as creatine (Cr) and two-thirds as phosphocreatine (PCR).
An average 150lb male has a creatine pool of approximately 120-140gms.Typically, humans manufacture about one gram/day of Cr, obtains one gram from food (muscle meats contain ~300-500 mg per 100gm serving), and loses about two grams per day. Therefore, under normal circumstances, creatine levels are fairly constant.
The phosphorylated form, creatine phosphate (PCR), provides an immediate energy source for the brain and muscles, and therefore, the primary rationales for supplementation are to increase, rapidly replete, and prolong this energy source to increase the metabolic capacity of these target tissues, such as the capability of a muscle to contract more powerfully longer and heal faster.
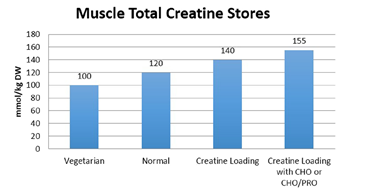
Thus, the goal of CS is to increase the muscle levels of Cr and speed the regeneration of PCR beyond what can practically be accomplished by diet alone. CS has been shown to increase SM total creatine content >15% and up to 24%, and >9% in the brain.
Increasing the body’s natural Cr content thru CS improves energy production that translates to improved activity outcomes in the short and long-term.
Want to learn why creatine is so important for athletes? Follow the link.
How does Creatine Monohydrate improve performance and hypertrophy?
CS helps you produce more energy for better workouts and recover faster/better
Acute performance: adenosine-triphosphate (ATP) is the energy molecule produced in the body that allows us to perform work. During all-out high-intensity activities lasting ~4-15seconds (e.g., jumping, sprinting, weightlifting, etc.) ATP is rapidly depleted but declines very little until stores of PCR are used.
Therefore, PCR, with its high-energy phosphoryl transfer potential, serves to maintain intracellular adenosine triphosphate (ATP) levels. CS significantly increases anaerobic capacity by raising the natural levels of PCR allowing intracellular concentrations of ATP to be maintained at higher levels for longer periods, permitting athletes to maintain greater training intensity and quality/quantity of each workout.
Maintaining higher quality workouts throughout an entire training period leads to greater overall performance gains immediately that also compound over time, including SM hypertrophy based on training protocols.
CS also delays fatigue by attenuating exercise-induced decreases in muscle pH, thereby buffering lactate and/or allowing less reliance on glycolysis. * Maximum amount of exertion a subject can sustain
Improved recovery leading to enhanced short and long-term gains: CS may also work through other unique muscle building mechanisms related to recovery, development and muscular adaptations during the supplementing phase.
These related mechanisms of CS may include changes in gene expression, satellite cell proliferation, insulin-like growth factor signaling, increase in growth hormone, alterations in myogenic transcription factors leading to a reduction in serum myostatin (muscle growth inhibitor), improved neuromuscular function (facilitating the reuptake of Ca2+ into sarcoplasmic reticulum), and as mentioned above, reduced exercise induced blood lactate.
Finally, CS may also participate in reducing certain types of muscle damage (not all ) from high intensity resistance training and endurance exercise allowing more complete recovery before subsequent exercise bouts.
CS increases the metabolic capacity of the target tissues, such as the capability of a muscle to contract more powerfully longer and also helps with faster complete recovery. Typical CS Results Using Standard Dosing Protocol (.045g/LB/d) in exercisers for 10 weeks: improved strength, body composition (LBM) and muscle size versus no supplementation.
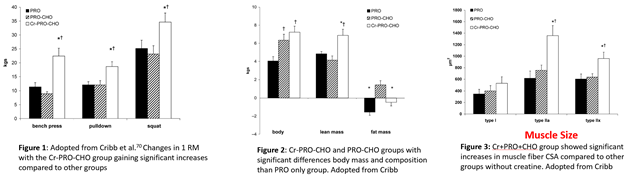
Bottom line: CS (Cr)-Protein (Pro)-Carbohydrate (CHO) provided greater desired adaptations than other groups with everything else equal in trained individuals.
For readers interested in a complete review on related CS study results click here Creatine Supplementation Review and International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine
Can CS improve aerobic performance?
Possibly through energy partitioning (where energy is drawn from), heat regulation and recovery
Relatively little has been studied or benefits quantified using CS in aerobic activities due to CS targeting the ATP-phosphocreatine energy system. If there is a benefit, it is probably related to a change in energy substrate utilization (when PCR levels are augmented by CS), at least during the early phase of aerobic activity that might help decrease time to exhaustion. To be sure, the coupling between PCR and VO2 kinetics is well documented.
Further, Roberts et al. found CS to augment muscle glycogen stores post exercise to potentially enhance the next bout of endurance activities. And finally, another mechanism in which CS may indirectly benefit aerobic activities is the ability of Cr to attenuate cardiovascular and thermoregulatory responses during prolonged exercise in the heat.
In aerobic/endurance activities, CS may improve energy usage, thermoregulation and overall recovery including glycogen restoration.
CS in Health Including Brain & Clinical Uses (pages 10-11 from Creatine Supplementation Review ,113-126)
Interested readers are referred to "Beyond Muscles: The Untapped Potential of Creatine” and “Beyond Sports” for more on CS and health including healthy aging. Below are highlights from current research referenced in the documents named above around CS in aging and health.
• Because there are high levels of Cr in the central nervous systems (CNS), CS may provide benefits to specific health conditions such as improvement in neurological & cognitive function including neurological disorders and trauma (studied in concussions).
• A review on CS effects on cognitive function showed higher brain Cr is associated with improved neuropsychological performance including cognitive processing, and CS can increase brain Cr and PCr.
• May be highly beneficial for women under certain conditions such as depression.
• CS can improve vascular function.
• CS offers protection against muscle wasting (sarcopenia).
• CS can improve bone remodeling in the elderly populations.
Note: although these are clinical applications, the usage helps confirm the strong health and safety profile of CS.
How do I use CS to get maximum results?
Effective Creatine dosing: load 5g 4xd for first 5-7d; 3-10g/d maintain till end of training phase cycle
Cr Loading phase: the most common and successful CS protocol starts with a loading phase of 20g/d of creatine monohydrate (CM) or 0.14 g CM/lb/d split into four daily intakes of 5g each for 5-7 days ingesting each dose with meal/shakes to improve Cr SM retention. Following the loading period, continue with the maintenance phase of 3-5g/d, or for larger athletes 5-10gm/d (or .04g/lb/d), for the duration of the supplementation period.
On training days, use one dose before workout and one after with meals/drinks. May mix with your pre/post training formula. On non-training days, take one dose with a morning meal and one dose with an evening meal if using 2 doses for maintenance, otherwise one dose with any meal. To maximize uptake and using multiple doses, CS intake should be spread as evenly as possible throughout the day with carbohydrate and/or protein containing meals or shakes (see figure below from Kreider et al). Some pre-workouts even contain creatine.
Bypassing the loading phase: some people choose not to do the loading phase and they are instructed to take the described maintenance dose daily (3-10gms based on weight shown above), which would take 21-28 days to reach maximum Cr SM saturation, thus delay the potential optimum ergogenic benefits.
The length of the supplementation period: would be based on the goal, but generally last 12-16 weeks and cycled as intense training is for competitive athletes throughout the year. However, daily continuous use for multiple years is not uncommon and considered safe when dosing properly in healthy individuals.CS used clinically or in aging populations would be decided by the attending qualified physician.
Best form of CS: is clearly creatine monohydrate (CM). While there are many different forms of creatine commercially available, at the time of this writing, CM, is the only form with sufficient safety and efficacy research to support the use of CS related to the claimed benefits since CM is the form used in virtually all peer review trials/studies.
Responders, partial and non-responders: while the effect size* or positive outcomes of CS studies is stronger that other ergogenic aids in specific activities described here, there is a smaller percentage of individuals that don’t respond as well as others (responders) and are often referred to as partial and non-responders. This sub-population that may demonstrate lesser improvements from CS, has been attributed to genetics (Type II fiber populations, gene polymorphisms, etc.), , diet (vegan/vegetarian vs. omnivore), , ineffective CS protocols (daily dosages, loading, etc.) and compliance.
*Effect size is a quantified measure of the experimental outcomes - in this case CS study effect versus placebos. The larger the effect size the stronger the relationship between two variables.
Creatine Supplementation Safety
The safety of short and long-term CS use is well established in healthy users using correct dosing. 25 years in over 1000 clinical trials, CS has been shown to be safe and effective when taken as directed in all healthy adult populations. Further, albeit fewer studies, CS also shows safety and efficacy in youth and adolescence trials.
Creatine and Creatinine and urine/blood tests. Creatinine is a normal by-product of Cr metabolism in all humans and therefore, due to the spontaneous conversion of creatine into creatinine, diet (e.g., high in animal protein), proper use of creatine supplements and/or vigorous exercise, can often lead to a creatinine level reading at or above the normal (>1.5 mg/dL), which in healthy persons, is a harmless temporary result.
Therefore, experts advise exercisers to not train or train lightly the day before a blood/urine test and CS users to cease supplementation 4 days before the tests, to avoid a potential “false positive” reading, and that healthy individuals may resume usage at any time following testing. Specific studies on CS, renal function and/or safety conclude that although Cr does slightly raise creatinine levels, there is no progressive effect to cause negative consequences to renal function and health in already healthy individuals when proper dosage recommendations are followed.
Creatine is a naturally occurring nitrogenous organic acid and therefore no precautions are known for healthy persons. However, as with any nitrogen containing acid (e.g., amino compounds such as amino acids/complete proteins), individuals with liver or kidney disease should avoid supplementation without supervision of a medical professional.
Creatine supplementation in youth and adolescence
General rule is ≥18 yrs unless a younger elite athlete is properly supervised with parent consent. The 18yrs or older label cautions on creatine products have to do with manufacturers shielding themselves from liabilities and not based on safety reasons since science has documented CS safety in all age groups as shown discussed above.
The latest position by the International Society of Sports Nutrition (ISSN) is the following: “If proper precautions and supervision are provided, creatine monohydrate supplementation in children and adolescent athletes is acceptable and may provide a nutritional alternative with a favorable safety profile to potentially dangerous anabolic androgenic drugs.
However, we recommend that creatine supplementation only be considered for use by younger athletes who: a.) are involved in serious/competitive supervised training; b.) are consuming a well-balanced and performance enhancing diet; c.) are knowledgeable about appropriate use of creatine; and d.) do not exceed recommended dosages”.
Enduring myths or misconceptions
Long-term use, muscle cramps, water retention and injury.
Muscle cramps and Hydration: CS has positive effects on muscle cramps and dehydration and in fact shown to reduce muscle cramps by 60%. Further, CS can increase total body water, reduce sweat rate, lower core temp and exercise heart rate,33 thus improves hydration and thermoregulation in athletes exercising in heat.
Water Retention: Creatine supplementation does not always lead to water retention, especially outside the muscle cell. Increases in muscle mass (MM) induced by Cr and training occurs without alteration of the ratio of intracellular water (ICW) to MM (i.e., there is a matching gain). Further, it has been shown that extracellular water (ECW) to MM ratio decreased suggesting improved MM quality – i.e., structural/size improvements (not just water).
Injury: athletes who supplement with creatine experience fewer musculoskeletal injuries and accelerated recovery time from injury.
Decreases kidney or liver functions: there are no negative effects on kidney or liver health in any age group of healthy users.
For more on Cr myths and misconceptions, readers are referred to the ISSN 2021 document titled, Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show?
Summary
Creatine monohydrate has been proven to be an extremely popular, safe and effective performance enhancing dietary supplement. CS clearly benefits specific athletes and activities and because Cr is involved in energy production in almost all tissues including skeletal, cardiac and smooth muscle, CS may offer a value to most anyone. PCr, provides an immediately available energy source for muscles and the brain, thus the primary rationale for CS.
The goal of CS is to increase the muscle (or other target tissues) levels of Cr to increase, and speed the regeneration, of PCr beyond what can practically be accomplished by diet alone to significantly enhance energy production. This practice would primarily benefit strength and power activities that are dependent on PCr as an energy source such as sprinting, weightlifting, jumping, and translate to other sports/activities that also require repetitive bursts of speed and power – i.e., specific intermittent athletes (team sports that combined intermittent aerobic and anaerobic activity such as football, baseball, rugby, soccer, hockey, etc.). Besides amplifying training outcomes, including increases in LBM, performance, strength, recovery and power for competitive athletes, CS has demonstrated similar results for older adults, which may lead to healthier aging and improved daily living.
CS has shown benefits in endurance/aerobic activities that may be related to a change in energy substrate utilization, at least during the early phase of aerobic activity that might help increase time to exhaustion. Additionally, CS’s well known hydrating properties may improve endurance performance during high heat conditions. And finally, CS is now being explored clinically for positive health outcomes such as improvement in neurological and cognitive function, offer protection against muscle and bone wasting (sarcopenia), neurological disorders, and trauma.
At the time of this writing, creatine monohydrate (CM) is the only evidence-based form of creatine proven for safety and efficacy. Young athletes who have not undergone puberty should not consider CS without qualified consultation.
Typical Use and Beneficiaries
Potential Beneficiaries (compared to non-supp state)
• Competitive athletes seeking to improve training outcomes related to increasing LBM and improving strength & power activities such as sprinting, weightlifting, and jumping. Benefits may translate to sports (“field of play”) requiring repetitive bursts of speed and power – i.e., specific intermittent athletes (team sports players such as football, baseball, soccer, rugby, hockey, lacrosse, etc.).
• Athletes with low creatine intake or biosynthesis who perform high intensity activity.
• Any exerciser desiring to break a performance plateau in any related activity (may improve motivation and activity longevity).
• Older adults seeking healthier aging and improved daily living as recommended by a qualified physician.
• Aerobic/endurance athletes to potentially delay fatigue especially under high heat conditions and assist post exercise glycogen re-synthesis & other recovery processes.
Safe and effect dosing
• Generally starts with a loading phase of 20g of creatine monohydrate (CM)/d, or 0.14g/lb split into four daily intakes of 5g each, followed by a maintenance phase of 3-10g/d (or 0.04 g/lb/d) based on body size for the duration of the supplementation period.
o Alternatively, start with the maintenance dose and continue throughout the supplement period – this method delays the ergogenic effect.
• The length of the supplementation period would be based on the goal, but generally last 12-16 weeks and cycled throughout the year in conjunction with intense training for competitive athletes.
• CS used clinically or in aging populations would be decided by the attending qualified physician.
• Each CM dose should be accompanied with some form of carbohydrate or protein to maximize SM uptake/retention.
References
Hickner R, Dyck D, Sklar J, Hatley H, Byrd P. Effect of 28 days of creatine ingestion on muscle metabolism and performance of a simulated cycling road race. J Int Soc Sports Nutr. 2010;7:26. doi: 10.1186/1550-2783-7-26
Safdar A, Yardley N, Snow R, Melov S, Tarnopolsky M. Global and targeted gene expression and protein content in skeletal muscle of young men following short-term creatine monohydrate supplementation. Physiol Genomics. 2008;32:219–228
Tyka AK, Chwastowski M, Cison T, Palka T, Tyka A, Szygula Z, Pilch W, Strzala M, Cepero M. Effect of creatine malate supplementation on physical performance, body composition and selected hormone levels in sprinters and long-distance runners. Acta Physiol Hung. 2015 Mar;102(1):114-22. doi: 10.1556/APhysiol.102.2015.1.12.
Deldicque L, Atherton P, Patel R, Theisen D, Nielens H, Rennie M, Francaux M. Effects of resistance exercise with and without creatine supplementation on gene expression and cell signaling in human skeletal muscle. J Appl Physiol. 2008;104:371–378
Hespel P, Derave W. Ergogenic effects of creatine in sports and rehabilitation. Subcell Biochem. 2007;46:245–259. doi:10.1021/bi061646s
Saremi A, Gharakhanloo R, Sharghi S, Gharaati M, Larijani B, Omidfar K. Effects of oral creatine and resistance training on serum myostatin and GASP-1. Mol Cell Endocrinol. 2010;317:25–30. doi: 10.1016/j.mce.2009.12.019
Bazzucchi I, Felici F, Sacchetti M. Effect of short-term creatine supplementation on neuromuscular function. Med Sci Sports Exerc. 2009;41:1934–41. doi: 10.1249/MSS.0b013e3181a2c05c
Dabidi Roshan V , Babaei H, Hosseinzadeh M, Arendt-Nielsen. The effect of creatine supplementation on muscle fatigue and physiological indices following intermittent swimming bouts. J Sports Med Phys Fitness. 2013 Jun;53(3):232-9
Northeast B, Clifford T. The Effect of Creatine Supplementation on Markers of Exercise-Induced Muscle Damage: A Systematic Review and Meta-Analysis of Human Intervention Trials. Int J Sport Nutr Exerc Metab. 2021 Feb 24;31(3):276-291. doi: 10.1123/ijsnem.2020-0282. PMID: 33631721.
Jooyoung Kim, Joohyung Lee, Seungho Kim, Daeyoung Yoon, Jieun Kim, Dong Jun Sung. Role of creatine supplementation in exercise-induced muscle damage: A mini review. Journal of Exercise Rehabilitation 2015;11(5):244-250
Antonio J, Candow DG, Forbes SC, Gualano B, Jagim AR, Kreider RB, Rawson ES, Smith-Ryan AE, VanDusseldorp TA, Willoughby DS, Ziegenfuss TN. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? J Int Soc Sports Nutr. 2021 Feb 8;18(1):13. doi: 10.1186/s12970-021-00412-w. PMID: 33557850; PMCID: PMC7871530.
Cribb PJ, Williams AD, Hayes A. A creatine-protein-carbohydrate supplement enhances responses to resistance training. Med Sci Sports Exerc. 2007;39:1960–1968. doi: 10.1249/mss.0b013e31814fb52a
Branch JD. Effects of creatine supplementation on body composition and performance: a meta análisis. Int J Sports Nutr Exerc Metabol. 2003;13:I198-122
Jones AM, Carter H, Pringle JS, Campbell IT (2002) Effect of creatine supplementation on oxygen uptake kinetics during submaximal cycle exercise. J Appl Physiol 92:2571–2577
Binzoni T, Ferretti G, Schenker K, Cerretelli P (1992) Phosphocreatine hydrolysis by 31P-NMR at the onset of constant-load. exercise in humans. J Appl Physiol 73:1644–1649
Lopez RM, Casa DJ, McDermott BP, Ganio MS, Armstrong LE, Marish CM (2009) Does creatine supplementation hinder exercise heat tolerance or hydration status? A systematic review. J Athl Train 44:215–2
R. Twycross‑Lewis, L. P. Kilduff, G. Wang, Y. P. Pitsiladis. The effects of creatine supplementation on thermoregulation and physical (cognitive) performance: a review and future prospects. Amino Acids DOI 10.1007/s00726-016-2237-9
Kerksick CM, Wilborn CD, Roberts MD, Smith-Ryan A, Kleiner SM, Jager R, Collins R, Cooke M, Davis JN, Galvan E, Greenwood M, Lowery LM, Wildman R, Antonio J, Kreider RB. ISSN exercise & sports nutrition review update: research & recommendations. J. Int. Soc. Sports Nutr. 2018;15:38–y.
Kreider RB, Jung YP. Creatine supplementation in exercise, sport, and medicine. J Exerc Nutr Biochem. 2011;15(2):53–69. 7. Hultman E, et al. Muscle creatine loading in men. J Appl Physiol (1985). 1996;81(1):232–7.
Buford T, Kreider R, Stout J, Greenwood M, Campbell B, Spano M, Ziegenfuss T, Lopez H, Landis J, Antonio J. International Society of Sports Nutrition position stand: creatine supplementation and exercise. J Int Soc Sports Nutr. 2007;4:6. doi: 10.1186/1550-2783-4-6
Ralf Jäger, Martin Purpura, Andrew Shao, Toshitada Inoue, Richard B, Kreider. Analysis of the efficacy, safety, and regulatory status of novel forms of creatine. Amino Acids (2011) 40:1369–1383 DOI 10.1007/s00726-011-0874-6
Kreider RB, et al. Long-term creatine supplementation does not significantly affect clinical markers of health in athletes. Mol Cell Biochem. 2003;244(1–2):95–104.
Writing Group for the NINDS Exploratory Trials in Parkinson Disease (NET-PD) Investigators, Kieburtz K, et al. Effect of creatine monohydrate on clinical progression in patients with Parkinson disease: a randomized clinical trial. JAMA. 2015 Feb 10;313(6):584-93. doi: 10.1001/jama.2015.120
Gualano B, Artioli GG, Poortmans JR, Lancha Junior AH. Exploring the therapeutic role of creatine supplementation. Amino Acids. 2010;38:31–44.
Lifanov D, Khadyeva MN, Rahmatullina LSh, Demenev SV, Ibragimov RR. Effect of creatine supplementation on physical performance are related to the AMPD1 and PPARG genes polymorphisms in football players. Ross Fiziol Zh Im I M Sechenova. 2014 Jun;100(6):767-76
Syrotuik DG, Bell GJ. Acute creatine monohydrate supplementation: a descriptive physiological profile of responders vs. nonresponders. J Strength Cond Res. 2004;18:610–617
Burke DG, Candow DG, Chilibeck PD, MacNeil LG, Roy BD, Tarnopolsky MA, Ziegenfuss T. Effect of creatine supplementation and resistance-exercise training on muscle insulin-like growth factor in young adults. Int J Sport Nutr Exerc Metab. 2008;18:389–398
Kaviani M, Shaw K, Chilibeck PD. Benefits of Creatine Supplementation for Vegetarians Compared to Omnivorous Athletes: A Systematic Review. Int J Environ Res Public Health. 2020 Apr 27;17(9):3041. doi: 10.3390/ijerph17093041. PMID: 32349356; PMCID: PMC7246861.
Jakobi J, Rice C, Curtin S, Marsh G. Contractile properties, fatigue and recovery are not influenced by short-term creatine supplementation in human muscle. Exp Physiol. 2000;85:451–460. doi: 10.1017/S0958067000020212.
Bemben MG, Witten MS, Carter JM, Eliot KA, Knehans AW, Bemben DA. The effects of supplementation with creatine and protein on muscle strength following a traditional resistance training program in middle-aged and older men. J Nutr Health Aging. 2010;14:155–159. doi: 10.1007/s12603-009-0124-8
Jagim, Andrew R et al. “Safety of Creatine Supplementation in Active Adolescents and Youth: A Brief Review.” Frontiers in nutrition vol. 5 115. 28 Nov. 2018, doi:10.3389/fnut.2018.00115
Felber S, Skladal D, Wyss M, Kremser C, Koller A, Sperl W. Oral creatine supplementation in Duchenne muscular dystrophy: a clinical and 31P magnetic resonance spectroscopy study. Neurol Res. 2000 Mar;22(2):145-50.
Tarnopolsky MA, Mahoney DJ, Vajsar J, Rodriguez C, Doherty TJ, Roy BD, Biggar D. Creatine monohydrate enhances strength and body composition in Duchenne muscular dystrophy. Neurology. 2004 May 25;62(10):1771-7.
Rebeca Lugaresi, Marco Leme, Vítor de Salles Painelli, Igor Hisashi Murai, Hamilton Roschel, Marcelo Tatit Sapienza, Antonio Herbert Lancha Junior, and Bruno Gualano. Does long-term creatine supplementation impair kidney function in resistance-trained individuals consuming a high-protein diet? J Int Soc Sports Nutr. 2013; 10: 26. Published online 2013 May 16. doi: 10.1186/1550-2783-10-26 PMCID: PMC3661339
Yoshizumi W, Tsourounis C. Effects of creatine supplementation on renal function. J Herb Pharmacother. 2004;4:1–7.
Thorsteinsdottir B, Grande J, Garovic V. Acute renal failure in a young weight lifter taking multiple food supplements, including creatine monohydrate. J Ren Nutr. 2006;16:341–345. doi: 10.1053/j.jrn.2006.04.025.
Pline K, Smith C. The effect of creatine intake on renal function. Ann Pharmacother. 2005;39:1093–1096. doi: 10.1345/aph.1E628
Poortmans J, Francaux M. Adverse effects of creatine supplementation: fact or fiction? Sports Med. 2000;30:155–170. doi: 10.2165/00007256-200030030-00002
Bizzarini E, De Angelis L. Is the use of oral creatine supplementation safe? J Sports Med Phys Fitness. 2004;44:411–416.
Kim HJ, Kim CK, Carpentier A, Poortmans JR. Studies on the safety of creatine supplementation. Amino Acids. 2011;40:1409–1418. doi: 10.1007/s00726-011-0878-2
1 Groff JL, Gropper SS, Hunt SM. Advanced Nutrition and Human Metabolism. St. Paul: West Publishing Company;1995. pp. 196- 197, 201.
Jagim, Andrew R, and Chad M Kerksick. “Creatine Supplementation in Children and adolescents.” Nutrients vol. 13,2 664. 18 Feb. 2021, doi:10.3390/nu13020664
Schilling B, Stone M, Utter A, Kearney J, Johnson M, Coglianese R, Smith L, O'Bryant H, Fry A, Starks M, et al: Creatine supplementation and health variables: a retrospective study. Med Sci Sports Exerc 2001, 33:183–188
Dalbo V, Roberts M, Stout J, Kerksick C: Putting to rest the myth of creatine supplementation leading to muscle cramps and dehydration. Br J Sports Med 2008, 42:567–573.
Chang, C. T., Wu, C. H., Yang, C. W., Huang, J. Y., and Wu, M. S. Creatine monohydrate treatment alleviates muscle cramps associated with haemodialysis. Nephrol.Dial.Transplant. 2002;17(11):1978-1981
Watson G, Casa D, Fiala K, Hile A, Roti M, Healey J, Armstrong L, Maresh C: Creatine use and exercise heat tolerance in dehydrated men. J Athl Train 2006, 41:18–29.
Ribeiro AS, Avelar A, Kassiano W, Nunes JP, Schoenfeld BJ, Aguiar AF, Trindade MCC, Silva AM, Sardinha LB, Cyrino ES. Creatine Supplementation Does Not Influence the Ratio Between Intracellular Water and Skeletal Muscle Mass in Resistance-Trained Men. Int J Sport Nutr Exerc Metab. 2020 Sep 11:1-7. doi: 10.1123/ijsnem.2020-0080. Epub ahead of print. PMID: 32916658.
Greenwood M, Kreider RB, Melton C, Rasmussen C, Lancaster S, Cantler E, Milnor P, Almada A. Creatine supplementation during college football training does not increase the incidence of cramping or injury. Mol. Cell. Biochem. 2003;244:83–8.
Greenwood M, Kreider R, Earnest CP, Rasmussen C, Almada AL. Differences in creatine retention among three nutritional formulations of oral creatine supplements. Journal of Exercise Physiology Online. 2003;6:37–43
Hespel P, Op't Eijnde B, Van Leemputte M, Urso B, Greenhaff PL, Labarque V, Dymarkowski S, Van Hecke P, Richter EA. Oral creatine supplementation facilitates the rehabilitation of disuse atrophy and alters the expression of muscle myogenic factors in humans. J. Physiol. 2001;536:625–33














