As a voice teacher, I was drawn to fitness to develop a sports-specific training protocol for singers. Corrective exercise techniques are often just as important as vocalises for helping my students to become the best singers they can be.
Excellent alignment is vital for breath management, volume and resonance when performing an opera aria, but resolving postural distortions can offer great benefits for voices of all kinds. Whether you use your voice for singing, public speaking, leading a group training class, or just in the course of normal conversation, a well-balanced musculature is the foundation for a well-projected, resonant voice, whereas postural distortions will lead to compromised vocal production (1,2).
People often believe that great singing voices are purely the result of genetics. In fact, a great deal can be done to free and enhance anyone’s natural voice through cultivating balance in the musculature that governs breathing and laryngeal function.
This post will examine the ways that some common postural distortions can impact the voice and propose ways that corrective exercise strategies can apply not only to resolving these distortions but also to improving key aspects of singing technique.
The Thoracic Diaphragm: Source of All Inspiration
The diaphragm is the primary muscle of inspiration. Shaped like a dome, it separates the thoracic and abdominal cavities. The crura of the diaphragm arise from the L1 - L3 vertebrae, and it inserts into the sternum and ribs 6 - 12. When you inhale, the diaphragm contracts and flattens, increasing the volume of the thoracic cavity and displacing the abdominal viscera.
 Lower Crossed Syndrome
Lower Crossed Syndrome
Postural distortions that impact the lumbar spine will compromise diaphragm function.
In lower crossed syndrome, the latissimus dorsi and erector spinae are shortened, exaggerating lumbar lordosis (1, 3). Decreased range of motion for the L1 - L3 vertebrae can lead to shortening of the crura of the diaphragm and vice-versa, limiting range of motion for the diaphragm and thus deep breathing (4).
The transverse abdominis (TA) and internal obliques play an expiratory role in breathing, acting as antagonists to the diaphragm; when lower crossed syndrome causes these muscles to become lengthened, they cannot optimally partner with the diaphragm and assist in expiration. Lengthening the lats and erector spinae and strengthening the TA and internal obliques will help re-establish full range of motion and optimal function of the diaphragm.
The Rib Cage: Full, Sustainable Expansion
The rib cage comprises 12 pairs of ribs, which are all attached to the spine posteriorly. Anteriorly, the highest ribs, 1 - 7, are attached to the sternum and ribs 8 - 10 are attached to the costal cartilages of the higher ribs; the lower ribs, 11 & 12, are the so-called “floating” ribs as they attach only to the spine and have no anterior attachment.
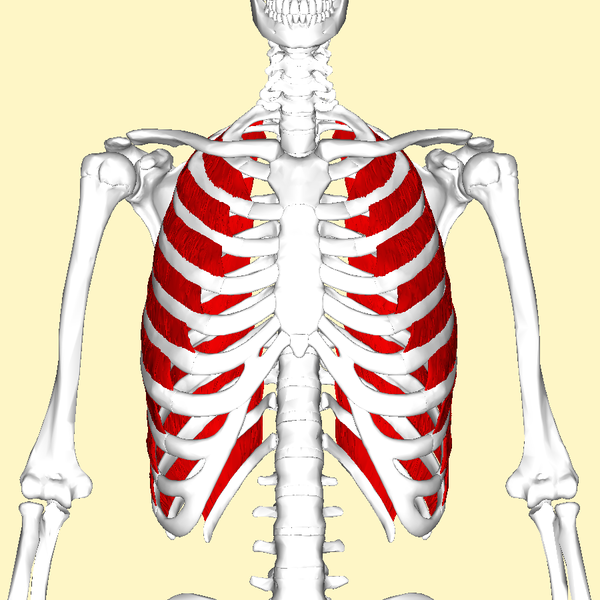 In normal breathing, the rib cage expands and the sternum elevates during inhalation; the ribs and sternum descend and settle during exhalation. While the external intercostal muscles are the primary movers of the ribs during inhalation, many other muscles assist with rib cage expansion and sternal elevation, including the rhomboids, middle and lower trapezius, and serratus anterior (5).
In normal breathing, the rib cage expands and the sternum elevates during inhalation; the ribs and sternum descend and settle during exhalation. While the external intercostal muscles are the primary movers of the ribs during inhalation, many other muscles assist with rib cage expansion and sternal elevation, including the rhomboids, middle and lower trapezius, and serratus anterior (5).
In breathing for classical singing, the ribs maintain an expanded position and the sternum remains elevated while singing/exhaling though sustaining an isometric contraction in the external intercostals, rhomboids, and the other muscles of costal inspiration.
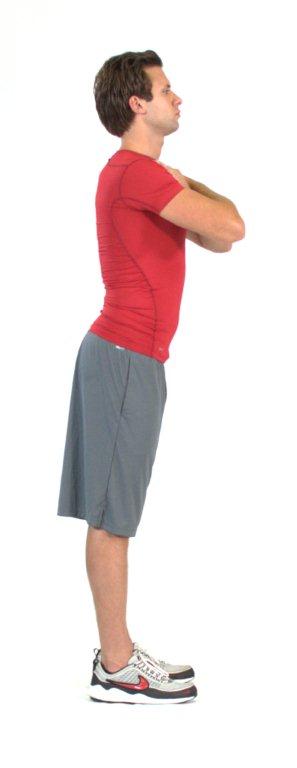
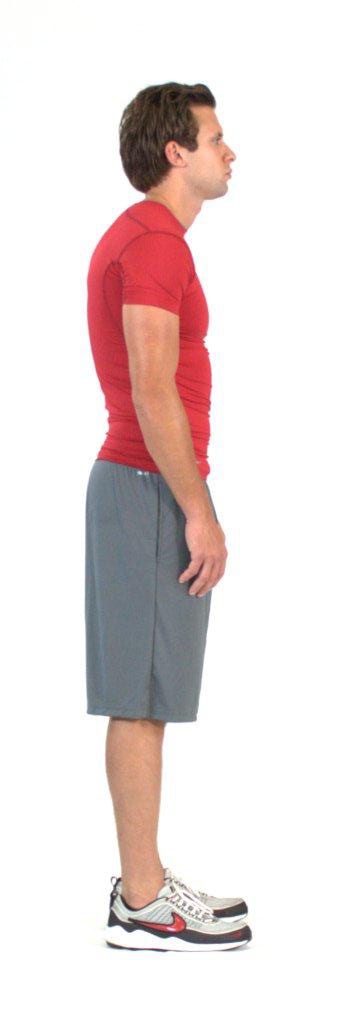 Upper Crossed Syndrome
Upper Crossed Syndrome
Postural distortions that impact the thoracic spine will impact costal respiration and sternal stability.
In upper crossed syndrome, tightness in the pectoral muscles and latissimus dorsi and weakness in the rhomboids and middle/lower trapezius result in an exaggerated kyphosis of the thoracic spine and a depressed position of the sternum (1,2). The sternum cannot fully ascend on inspiration, and expansion of the rib cage is limited anteriorly.
Lengthening the lats and pecs and strengthening the rhomboids and middle and lower trapezius will restore full range of motion in the sternum and rib cage and promote fuller costal breathing. Singers must cultivate exceptional strength and coordination in the rhomboids, middle and lower trapezius, and other muscles involved in scapular retraction, as well as the external intercostals, in order to maintain an elevated sternum and an expanded rib cage while singing/exhaling.
The Larynx: Freedom through Stability
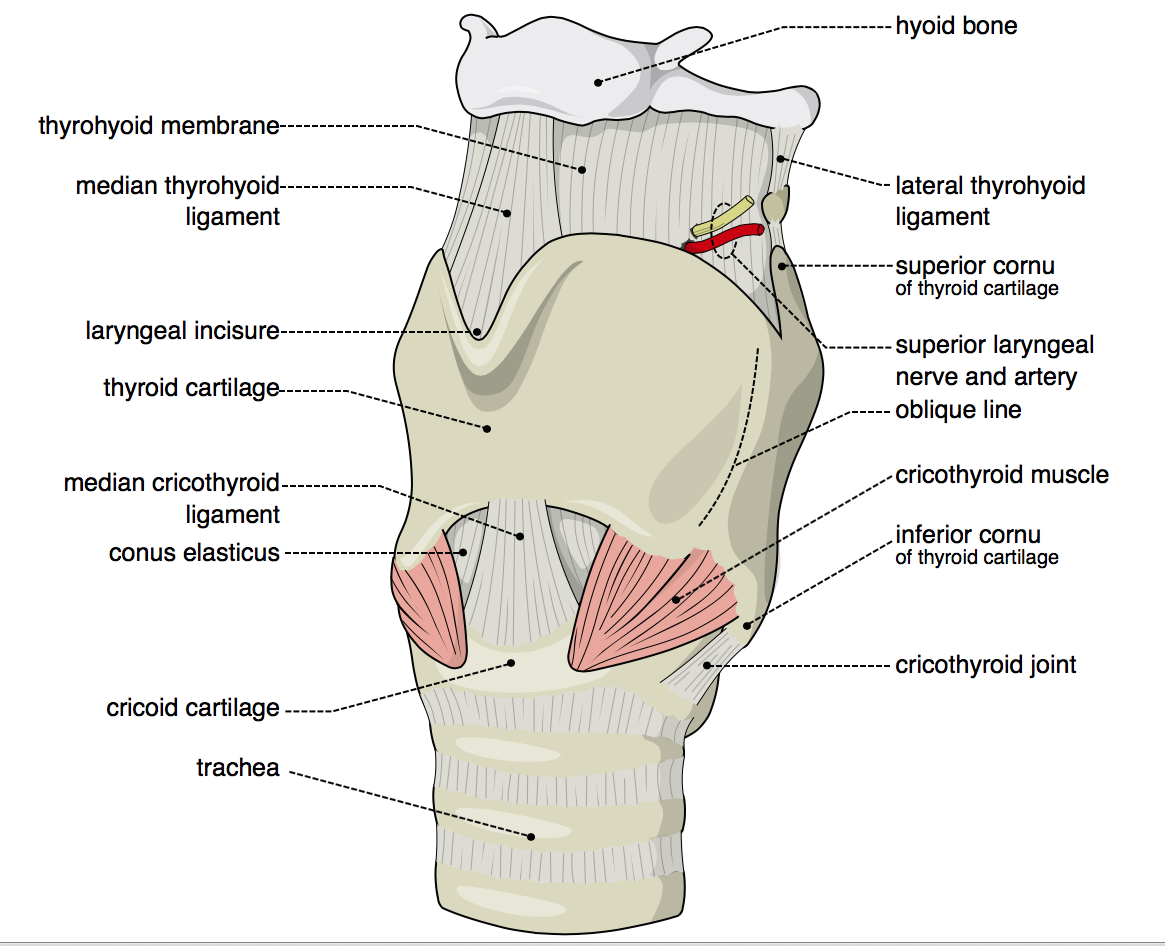 The larynx comprises the thyroid and cricoid cartilages. Housed within are the vocal folds, which vibrate to produce speech and singing, as well as structures that adjust their pitch, registration and volume. The larynx is suspended from the hyoid bone; the hyoid bone is anterior to vertabra C3 and the larynx occupies space in the throat anterior to vertebrae C4 - C6.
The larynx comprises the thyroid and cricoid cartilages. Housed within are the vocal folds, which vibrate to produce speech and singing, as well as structures that adjust their pitch, registration and volume. The larynx is suspended from the hyoid bone; the hyoid bone is anterior to vertabra C3 and the larynx occupies space in the throat anterior to vertebrae C4 - C6.
Postural distortions that impact the cervical spine will impact laryngeal stability and freedom.
To tune the voice, the cartilages of the larnyx must be free to tilt front to back at the cricothyroid joint. In upper crossed syndrome, exaggerated lordosis of the cervical spine caused by a shortening of the upper trapezius, levator scapulae, sternocleidomastoid and scalenes can compress the room available in the neck that the larynx requires in order to tilt freely.
To access optimal resonance, the larynx must rest in a stable, low position in the throat. In upper crossed syndrome, the sternohyoid and sternothyroid are lengthened and cannot adequately stabilize the larynx. Lengthening the cervical extensors and strengthening the deep cervical flexors will alleviate exaggerated lordosis of the cervical spine, creating conditions where the larynx may tilt freely and the laryngeal stabilizers can properly engage.
Apply corrective exercise tools to resolve postural distortions and your instrument can become the vocal equivalent of a Stradivarius.
References:
- Clack MA, Lucett SC. (2011). NASM Essentials of Corrective Exercise Training. Baltimore, MD: Lipincott, Williams & Wilkins, 2011.
- Dayme, Meribeth Bunch. Dynamics of the singing voice. Springer Science & Business Media, 2009.
- Clark MA, Sutton BG, Lucett SC. (2014). NASM Essentials of Personal Fitness Training, 4th ed., Rev. Burlington, MA: Jones & Bartlett Learning.
- Collins, Steve. “Anterior Pelvic Tilt (A Paradox, A Question, Some Possible Answers)”. Lost in Fitness. September 2, 2012. http://lostinfitness.blogspot.com/2012/09/anterior-pelvic-tilt-paradox-question.html
- Calais-Germain, Blandine. Anatomy of Breathing. Eastland Press, 2006.