In 2007, a group of physical therapy scholars published a scientific paper that formalized a musculoskeletal examination and treatment paradigm called the Regional Interdependence Model (RI) (Wainner et al., 2007).
Let's explore further how the RI model factors into the updated NASM CES Course, and Corrective Exercise as a whole.
What is the regional interdependence model?
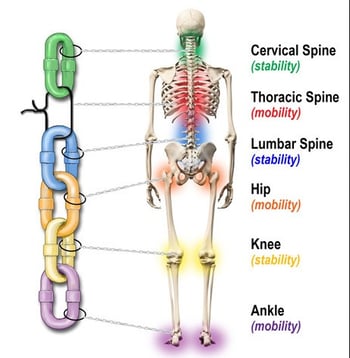
The RI model has an objective of identifying unrelated impairments in remote anatomical regions that may contribute to the primary source of pain or movement dysfunction (Figure 1) (Cheatham & Kreiswirth, 2014; Wainner et al., 2007). For example, an observed movement impairment at the knee could be influenced by factors (e.g., mobility limitations) at the hip joint above or below the ankle/foot.
How does the regional interdependence model differ from other models?
The RI model differs from more traditional treatment models by focusing on the kinetic chain, which is the interrelated groups of body segments, joints, and soft tissues that connect them, and not just one body region in isolation.
Historically, examination and treatment models focused on one anatomical body region and failed to acknowledge that areas above or below could be associated with the primary site of impairment (Cheatham & Kreiswirth, 2014).
The RI model opens the door for a more comprehensive and organized assessment of the human movement system (HMS).

Since the RI model’s inception, over a hundred studies have utilized the concept for HMS examination and rehabilitation strategies for different conditions.
In 2013, the original RI model was updated and expanded for medical professionals to consider that any HMS impairment involves a response from multiple systems of the body.
For example, an ACL tear can become a musculoskeletal, neurophysiological, somatovisceral, and/or biopsychosocial issue (Sueki et al., 2013).
RI Model and the NASM Certified Professional
Recognition of the interdependence of the different body regions has been around for years with the human kinetic chain (Karandikar & Vargas, 2011). For example, the concept of the kinetic chain and underlying principles form the foundation from which the NASM OPT Model and corrective exercise continuum were developed.
While fitness professionals are proficient at observing and correcting the HMS during physical activity to ensure proper movement, more focus may be placed on the kinesiology and biomechanics of global movement (e.g., proper squat form, etc.) without considering the influence of impaired body regions when poor movement efficiency is observed (Karandikar & Vargas, 2011).
This is where the RI model may offer value for fitness professionals. The original RI model fits well within the scope of practice and corrective exercise approach and may help fitness professionals to 1) first identify the primary impairment in the HMS and then 2) consider impairments at remote regions above or below that may be associated with the primary issue and 3) identify any potential HMS issues that require a referral to a licensed professional.
The RI model within the corrective exercise framework helps the fitness professional more readily identify “weak links” in the human kinetic chain (Figure 2).
The RI Model and Corrective Exercise
The RI Model is a foundational part of the updated 2020 Corrective Exercise Specialist (CES) course. There is a need for fitness professionals to take a more comprehensive and organized approach to HMS dysfunction.
The RI model within the corrective exercise framework provides the tools to identify kinetic chain impairments further and develop corrective programming. This can be accomplished with the corrective exercise assessment flow and corrective exercise programming continuum.
For the CES assessment, the RI model is utilized through observation of the five kinetic chain checkpoints (ankles/feet, knees, LPHC, thoracic spine & shoulders, and cervical spine & head), which are critical regions of the body's kinetic chain. These checkpoints are often observed during the CES static assessment (e.g., posture), movement assessment (e.g., OHSA, transitional, dynamic, loaded), and mobility assessment. The RI model reminds the fitness professional to consider the interdependence of the kinetic chain checkpoints during the assessment process.
|
Trainer Tip |
|
Upon completing the CES assessment, the fitness professional may want to rank the five kinetic chain checkpoints from the high to low priority (1-high, 5-low) regarding impairments. The checkpoint with the most significant issue/s (e.g., highest priority) can address first followed by the others. This helps organize the assessment results and systematically addresses each issue through corrective exercise programming for each client. |
For the Corrective Exercise Continuum (CEx), fitness professionals can integrate the RI model into their client programming. The four steps in the CEx include: inhibit, lengthen, activate, integrate.
For example, the fitness professional can address the kinetic checkpoint with the highest importance (e.g., primary impairment) first and then focus on the other checkpoints (above and below) to make sure the kinetic chain moves efficiently. However, it is not uncommon to simultaneously address multiple checkpoints along the kinetic chain, especially when the client is ready for integrative movements involving various checkpoints (Sciascia & Cromwell, 2012). Thus, any step in the CEx can be applied to one or more checkpoints.
|
Trainer Tip |
|
The CEx can be applied to one or more checkpoints based upon their high to low rankings. This helps to prioritize the client’s program and provide an efficient corrective action plan. This approach represents the RI model. |
Conclusion
The RI model is a foundational part of the CES assessment and the CEx programming framework. The fitness professional can use the kinetic chain checkpoints to organize client assessment and exercise programming. The RI model reminds fitness professionals to address any “weak links” in the human kinetic chain.
The updated 2020 CES materials provide a more in-depth discussion, organization, and application of these concepts. Please reach out to a NASM advisor with any questions about the updated CES.
References
Cheatham, S., & Kreiswirth, E. (2014). The Regional Interdependence Model: A Clinical Examination Concept. 19(3), 8. https://doi.org/10.1123/ijatt.2013-0113
Karandikar, N., & Vargas, O. O. (2011, Aug). Kinetic chains: a review of the concept and its clinical applications. Pm r, 3(8), 739-745. https://doi.org/10.1016/j.pmrj.2011.02.021
Sciascia, A., & Cromwell, R. (2012). Kinetic chain rehabilitation: a theoretical framework. Rehabil Res Pract, 2012, 853037-853037. https://doi.org/10.1155/2012/853037
Sueki, D. G., Cleland, J. A., & Wainner, R. S. (2013, May). A regional interdependence model of musculoskeletal dysfunction: research, mechanisms, and clinical implications. The Journal of manual & manipulative therapy, 21(2), 90-102. https://doi.org/10.1179/2042618612y.0000000027
Wainner, R. S., Whitman, J. M., Cleland, J. A., & Flynn, T. W. (2007, Nov). Regional interdependence: a musculoskeletal examination model whose time has come. The Journal of orthopedic and sports physical therapy, 37(11), 658-660. https://doi.org/10.2519/jospt.2007.0110